
The first time my lower back locked up, I did what everyone does — I Googled stretches, tried a few, felt slightly better, then woke up the next morning worse than before. That cycle lasted months. Maybe yours has too.
If you’re looking to learn how to treat back pain and sciatica at home, the short answer is this: most people fail not because they don’t try hard enough, but because they keep doing things — specific stretches, specific postures, specific daily habits — that actively prevent the spine from healing. Back pain relief is less about adding the right exercises and more about stopping the wrong ones first. Once you remove those constant re-injury triggers and replace them with a small set of evidence-based movements, the spine finally gets the environment it needs to recover.
- Most common back stretches people do actually increase disc pressure and make herniation worse over time
- The order matters: eliminate causes first, then add corrective exercises — reversing that order prolongs pain
- Sciatica responds to specific nerve mobilization techniques, not generic leg stretches
What “Treating Your Own Back Pain” Actually Means
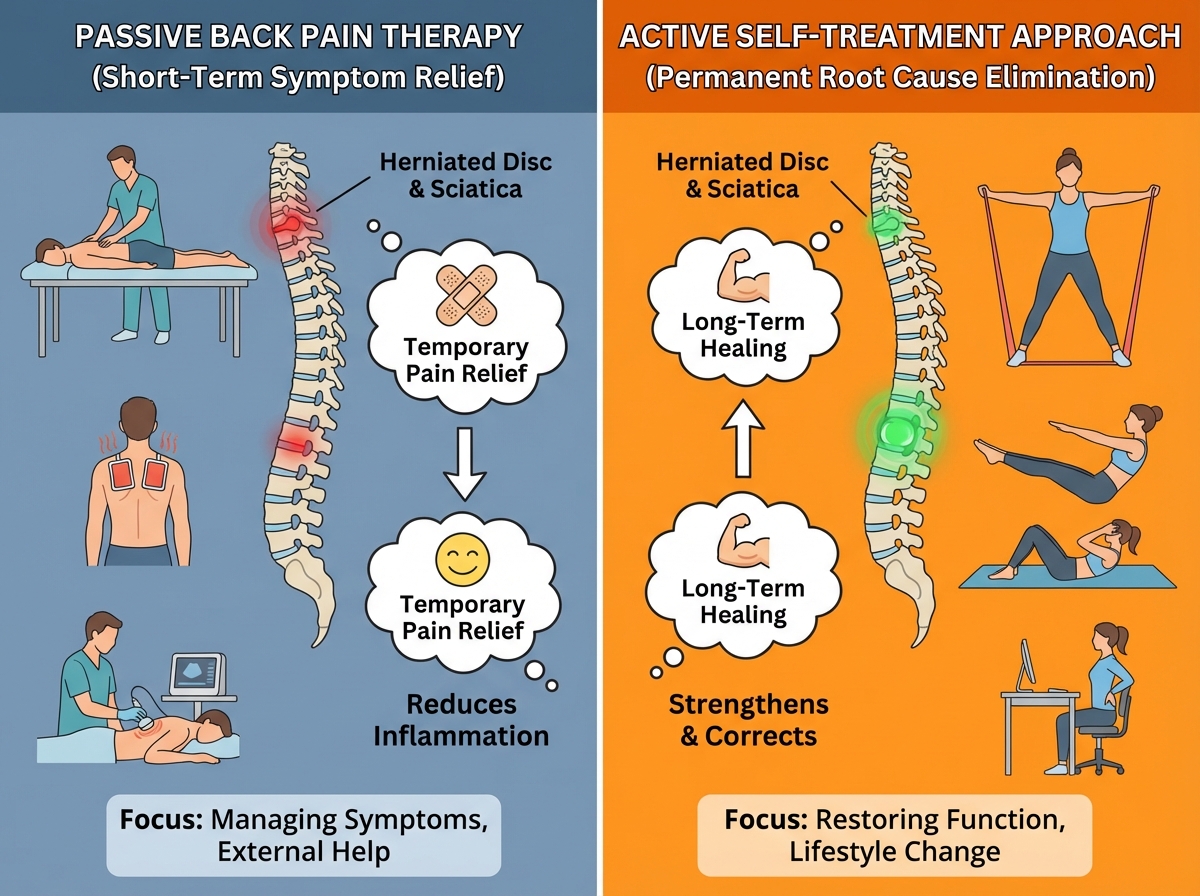
Self-treatment for back pain doesn’t mean ignoring serious symptoms or refusing medical care. It means becoming an active participant in your own recovery instead of a passive recipient of someone else’s treatment. The distinction is important because no amount of external therapy — massage, chiropractic, injections — holds if you walk out of the clinic and immediately resume the postures and movements that caused the problem.
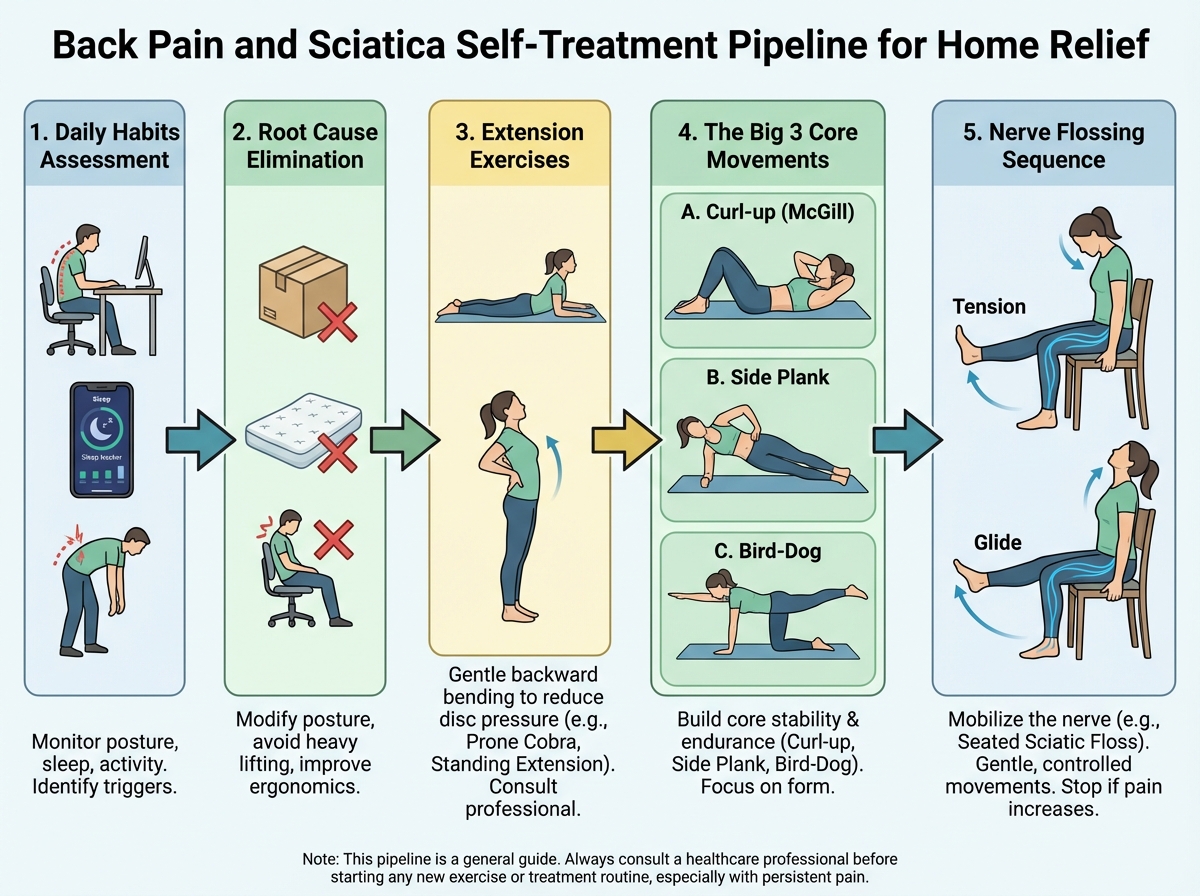
For someone dealing with lower back pain, a bulging disc, a pinched nerve, or sciatic nerve pain running down into the leg, the self-treatment framework covers three things: identifying and stopping what’s damaging the spine daily, performing specific exercises that decompress the disc and restore movement, and building the core stability that protects against future episodes.
| Approach | What It Targets | Works Without Addressing Root Cause? |
|---|---|---|
| Passive therapy (massage, chiro) | Symptom relief | Temporary — pain returns |
| Generic stretches (knee-to-chest, seated forward fold) | Perceived tightness | Often makes disc problems worse |
| Evidence-based self-treatment | Root cause + corrective exercise | Yes — designed to work independently |
| Surgery / medication | Structural or pain signal | Sometimes necessary, often avoidable |
Three things that make self-treatment for back pain different from generic advice:
- It requires identifying your personal pain triggers — not applying a generic protocol
- The exercises are sequenced deliberately — the decompression work comes before the stability work
- It treats sciatica and referred nerve symptoms as a separate but connected problem requiring its own technique
Why You’re Probably Making Your Back Worse Right Now
This was the hardest thing to accept: the stretches I’d been doing for years — the ones that felt like they were helping — were likely making things worse. The classic knee-to-chest pull, the seated toe-touch, the prolonged forward bend — these all load the posterior disc in ways that, for someone with a bulge or herniation, increase the pressure on already compromised tissue. The relief you feel is real, but it’s temporary, and the structural situation underneath is quietly deteriorating.
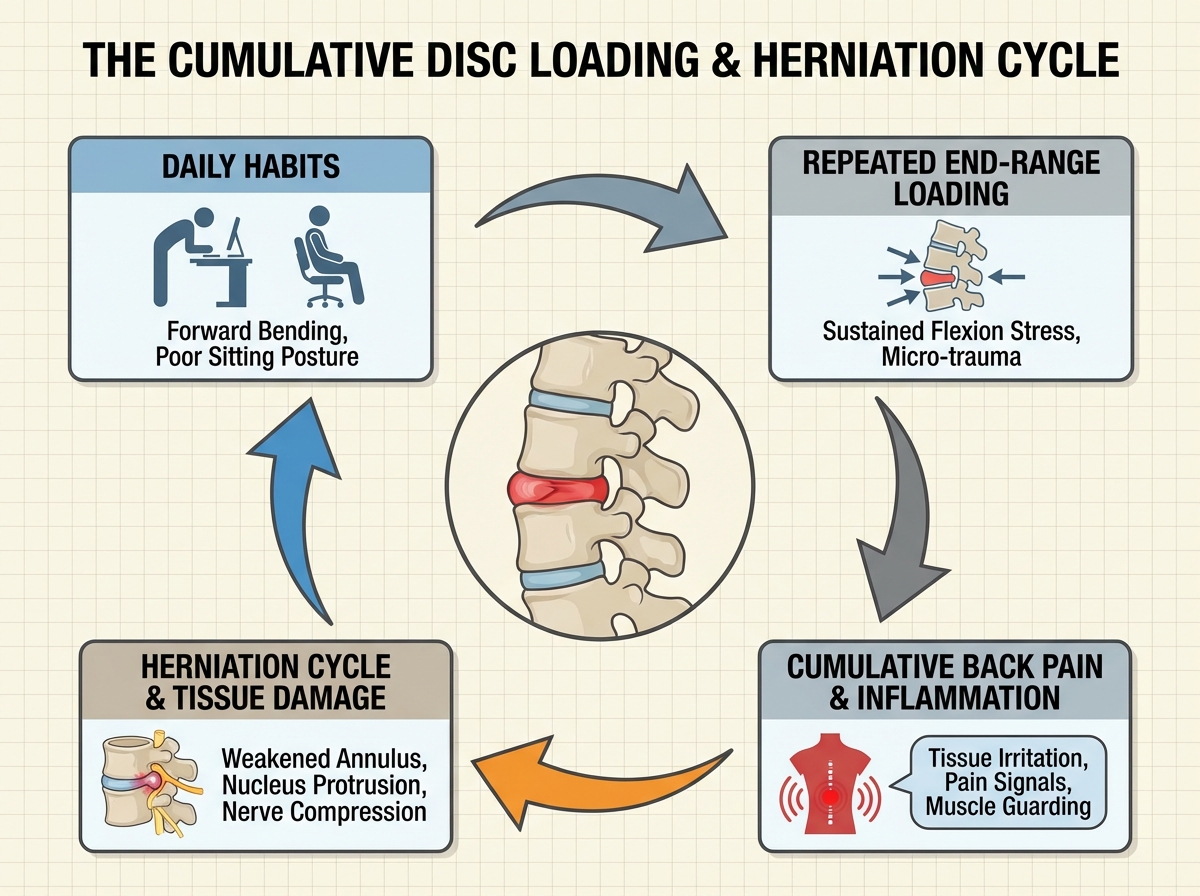
The biggest mistake people make when dealing with back pain is treating every session of pain as a separate, random event instead of recognizing it as the cumulative result of dozens of small daily decisions. The way you sit at a desk, the way you bend to pick something up, the way you stand in the kitchen — all of it adds up. Some positions and movements cause what researchers call “repeated end-range loading” of the disc, and if you’re doing those things twenty times a day, no exercise routine in the evening is going to overcome that.
The moment things started to shift for me was when I stopped asking “what can I do to fix my back” and started asking “what am I doing that’s preventing it from healing.” That’s not a motivational reframe — it’s a structural one. The spine wants to heal. Discs have the capacity to reabsorb and recover. The question is whether your daily mechanics are giving it any chance to do so.
The Exercises That Actually Decompress the Disc
Once you’ve started auditing and reducing the movements that load the disc, you can begin the work that actually reverses compression. The foundational movement here is lumbar extension — specifically, prone press-ups where you lie face down and gently extend the lower back while the hips stay on the ground. The mechanism isn’t mysterious: extension in the prone position tends to migrate disc material anteriorly, away from the nerve roots, and repeated gentle repetitions over time help centralize and reduce symptoms.
The first time I tried this, it felt almost too simple. Lie on your stomach, push your upper body up, breathe. But what I noticed over a few days was that the radiating sensation into my leg — that deep, electric ache that runs from the glute to the calf — started to fade. Not immediately. Not dramatically. But it shortened. The pain that was in my foot moved to my knee, then to my hip, then disappeared. That centralization pattern is actually a sign it’s working.
If you can’t lie down because extension hurts in that position, there are standing variations. If extension makes things worse regardless, that’s information too — it may point to a different mechanical presentation, like stenosis, which requires a different approach. The exercise isn’t universal, but for most disc-related lower back pain, it’s the most evidence-supported starting point available.

Walking, Posture, and the Underrated Daily Tools
Walking tends to get dismissed because it feels too passive, too ordinary. But for lower back pain, walking is genuinely therapeutic — it creates rhythmic, low-load movement through the lumbar spine, activates the stabilizing muscles without compressing the disc, and keeps the facet joints mobile. The key is how you walk, not just that you walk.
Standing posture matters as much as sitting posture, and both require a mild lumbar curve — not a flat back, not an exaggerated arch, but a natural, supported curve that keeps the disc loading symmetrical. If standing aggravates your pain, there are positional adjustments — a foot up on a low surface, gentle weight shifting — that reduce that load. If walking itself causes pain that spreads or increases, that changes the protocol significantly and suggests the nerve component needs addressing before general movement increases.
The detail that surprised me most was how much the position while waiting matters — standing at a counter, sitting in a car for thirty minutes, sleeping on a surface that lets the spine sag. These aren’t dramatic events, but they accumulate. The first week I tracked every situation where I felt my back position change, I found nine or ten small recurring patterns that I hadn’t noticed before. Fixing three of them made a visible difference within days.
The Big 3: Core Stability Without Spinal Flexion
At some point in the recovery process, the work shifts from decompression to stabilization. This is where the “Big 3” movements come in — a set of exercises designed to build the endurance of the muscles that protect the lumbar spine, without putting the spine into the loaded flexion that standard crunches and sit-ups require. These aren’t optional additions once you feel better. They’re the reason the improvement holds.
The three movements are the modified curl-up (a small, controlled lift that avoids full spinal flexion), the side bridge (which loads the lateral stabilizers without compressing the disc), and the bird-dog (an opposite arm-leg extension from all-fours that trains the deep stabilizers under minimal load). None of them look impressive. None of them create the burn that people associate with a “core workout.” That’s exactly the point — the goal is endurance in a neutral spine position, not strength through a loaded range.
The cat-camel movement pairs well here, not as a strengthening exercise but as a motion-prep technique — cycling through spinal flexion and extension gently before loading the spine helps restore movement quality and reduces stiffness. Think of it as greasing the joint, not training the muscle.

For anyone dealing with persistent lower back pain and sciatica exercises, the sequencing of these movements matters more than the movements themselves. Extension work first, then stabilization work second. Doing them in the wrong order — trying to strengthen a spine that’s still under constant compressive load — produces inconsistent results at best.
What Sciatica Actually Needs (It’s Not a Leg Stretch)
Sciatica is one of the most misunderstood pain patterns people try to self-manage. The shooting or aching sensation down the leg, the numbness in the foot, the burning in the glute — it feels like the leg is the problem, so people stretch the leg. Hamstring stretches, piriformis stretches, IT band work. Some of it might feel temporarily relieving, but it’s not addressing what’s actually happening.
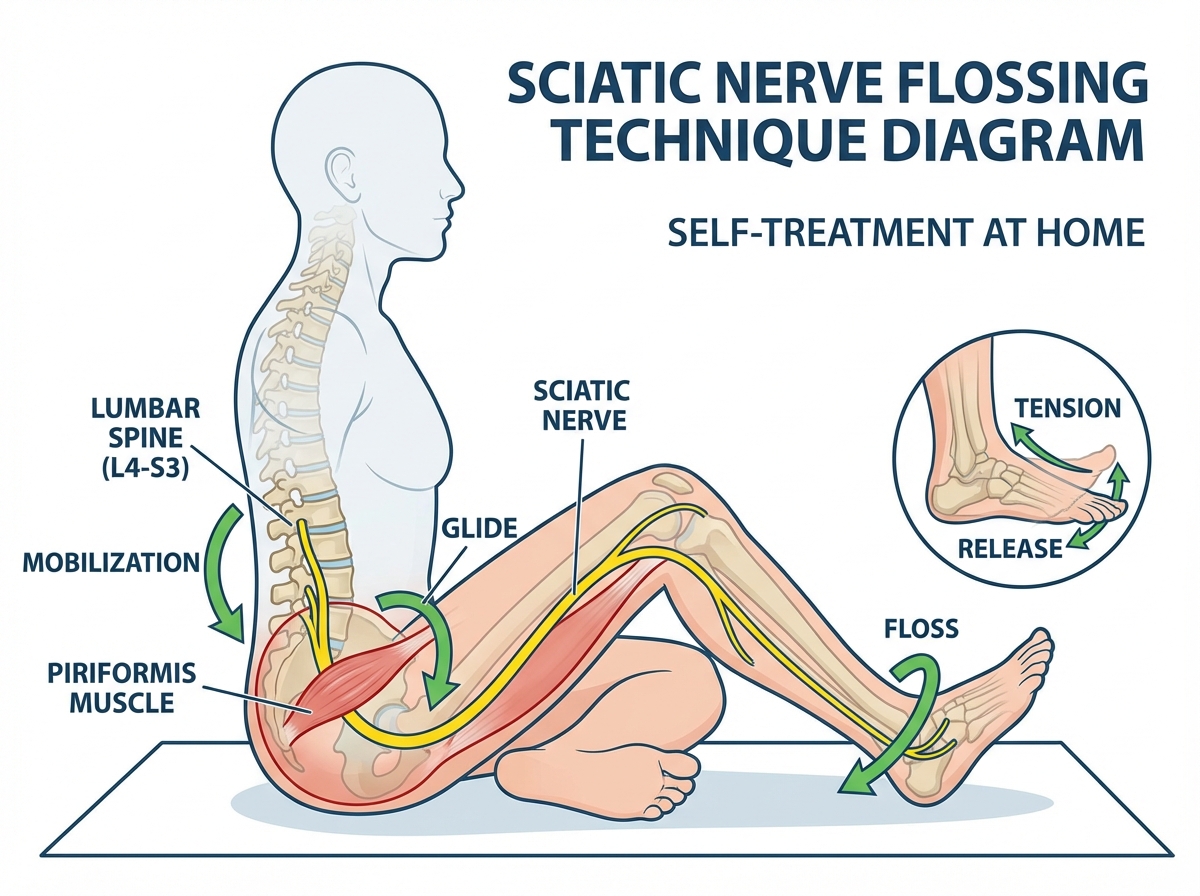
The sciatic nerve originates from the lumbar spine and travels down through the pelvis and leg. When it’s irritated — either from compression at the disc level or from mechanical tension along its path — it needs movement, not stretch. Specifically, it responds to nerve flossing, a technique that gently mobilizes the nerve through its full range of travel without putting it under sustained tension. The technique involves controlled, rhythmic movements that slide the nerve through surrounding tissue rather than pulling it taut.
The first time I tried nerve flossing after weeks of piriformis stretching that wasn’t helping, the difference was noticeable within a few sessions. Not cured — but the quality of the sensation changed. It became less electric, more dull. Less constant, more intermittent. That shift in symptom quality is often the first real sign that the nerve is responding rather than remaining in a state of ongoing irritation.
How Long Does Back Pain Relief Actually Take
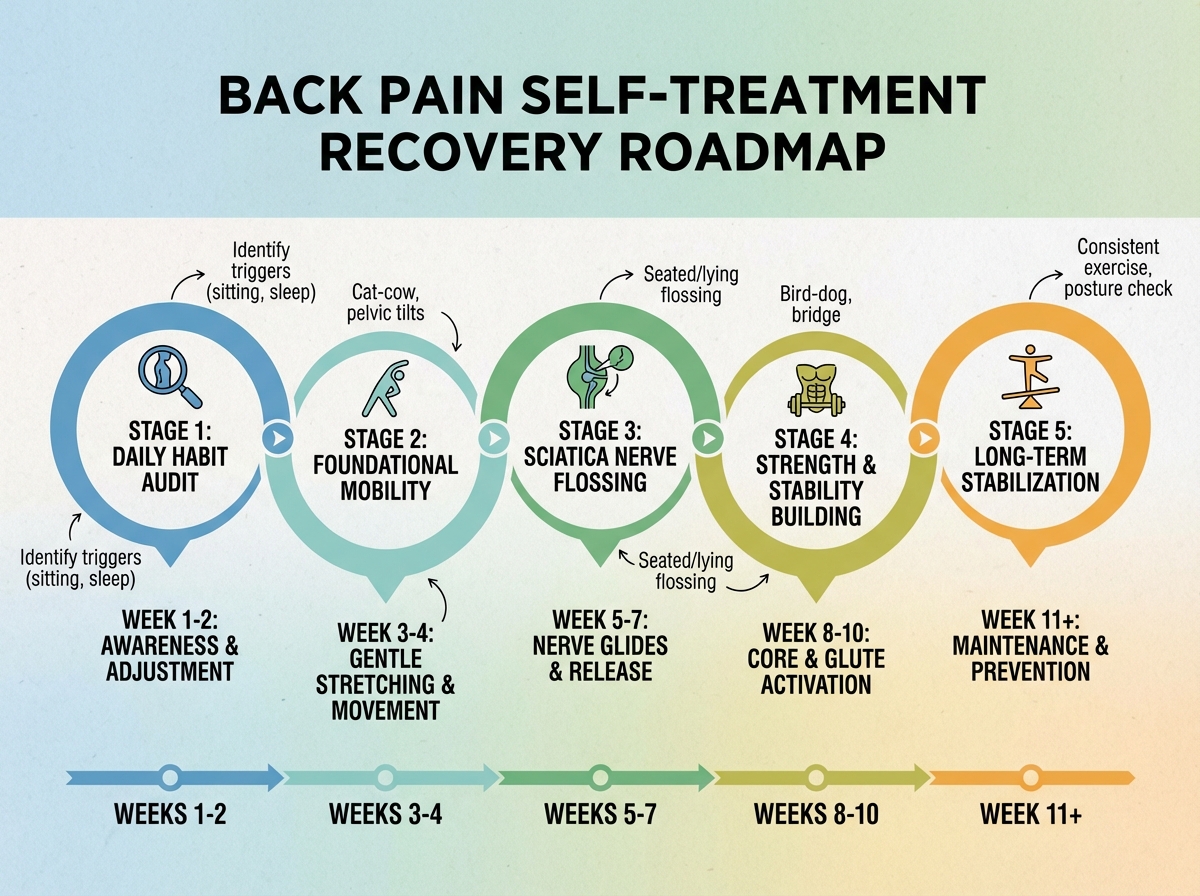
| Stage | What’s Happening | Typical Time |
|---|---|---|
| Cause identification | Auditing daily habits, stopping harmful movements and stretches | Days 1–7 |
| Acute symptom reduction | Extension exercises, walking modifications, positional corrections | Weeks 1–3 |
| Centralization of symptoms | Radiating pain pulls back toward the spine as disc pressure decreases | Weeks 2–5 |
| Stabilization work | Big 3 exercises introduced, core endurance built | Weeks 4–8 |
| Maintenance and prevention | Consistent daily habits, occasional flare management | Ongoing |
| Total to meaningful relief | 4–8 weeks for most people |
Order matters more than speed here — trying to rush into stabilization exercises before the acute compression phase is managed typically sets people back. If your timeline runs longer than the estimate, that’s not failure — it usually means the cause-elimination phase needed more attention than expected, not that the approach isn’t working.
The Tennis Ball, the Foam Roller, and What Soft Tissue Work Can Actually Do
Self-myofascial release — using a tennis ball or similar tool to apply pressure to tight tissue — has a specific and limited role in back pain management. It works well for the muscles surrounding the spine, particularly the glutes, the piriformis, and the thoracic paraspinals. It does not work on the disc. Applying direct pressure to an acutely inflamed lumbar area can increase irritation.
The tennis ball technique for the glute and hip musculature is genuinely useful as a complement to the main protocol — particularly for people whose sciatica involves tension in the piriformis, where the sciatic nerve passes close to or through the muscle belly. The pressure-hold technique, where you find a tender point and breathe through it rather than rolling back and forth, tends to produce better tissue release than rapid rolling.
The distinction I’d make is this: soft tissue tools are useful for managing peripheral tension and maintaining mobility, but they cannot substitute for the mechanical work that actually changes the disc’s position or the stability work that protects the spine. Use them as support, not as the primary strategy.

What Changes After You Understand All of This
The shift that happens when you finally connect the mechanics — when you understand exactly why forward bending loads the posterior disc, why extension relieves it, why the nerve responds to flossing and not to stretching — is that you stop being afraid of your back. Fear of movement is one of the most underappreciated drivers of chronic back pain. People with persistent pain often unconsciously limit their movement, which accelerates muscle atrophy and reduces disc nutrition, which makes the underlying problem worse.
Knowing the mechanism doesn’t just give you a protocol. It gives you decision-making capacity in real time. When something hurts, you can ask: is this extension-sensitive or flexion-sensitive? Is this nerve pain or muscle pain? Is what I’m about to do going to centralize or peripheralize my symptoms? Those aren’t abstract questions — they’re practical filters that let you manage your own back intelligently instead of reacting to it blindly.
That clarity is the actual endpoint. Not just a pain-free week, but a permanent shift in your relationship with your own spine — knowing what it needs, what it doesn’t, and how to respond when things flare up, because they sometimes will.
Stop all knee-to-chest and seated forward-bend stretches immediately — for disc-related pain, these increase posterior disc pressure and directly counteract the decompression work you’re trying to do.
Track your pain centralization daily — note whether radiating symptoms are moving closer to the spine or further away; centralization means the approach is working, peripheralization means something needs to change.
Do prone press-ups at the first sign of a flare — ten repetitions with a brief pause at the top is more effective done early than waiting until the pain escalates.
Build your Big 3 around endurance, not reps — hold the bird-dog for ten seconds per side, the side bridge for ten seconds, the modified curl-up for ten seconds; increase hold time before adding reps.
Audit one new daily position every three days — sitting at a desk, loading a dishwasher, sleeping position, driving posture; most people find their main re-injury trigger within the first ten days of this audit.
Use nerve flossing before static stretching for sciatica — mobilize the nerve first through gentle rhythmic movement, then address any remaining soft tissue tension; the reverse order often irritates an already sensitized nerve.
Restore your lumbar curve in sitting before doing anything else — a rolled towel or lumbar support positioned at the belt line changes the disc loading mechanics of every hour you spend at a desk.
Treat a pain-free day as information, not permission to stop — the structures that caused the problem are still adapting; the absence of pain means the protocol is working, not that the work is finished.
Leave a Reply