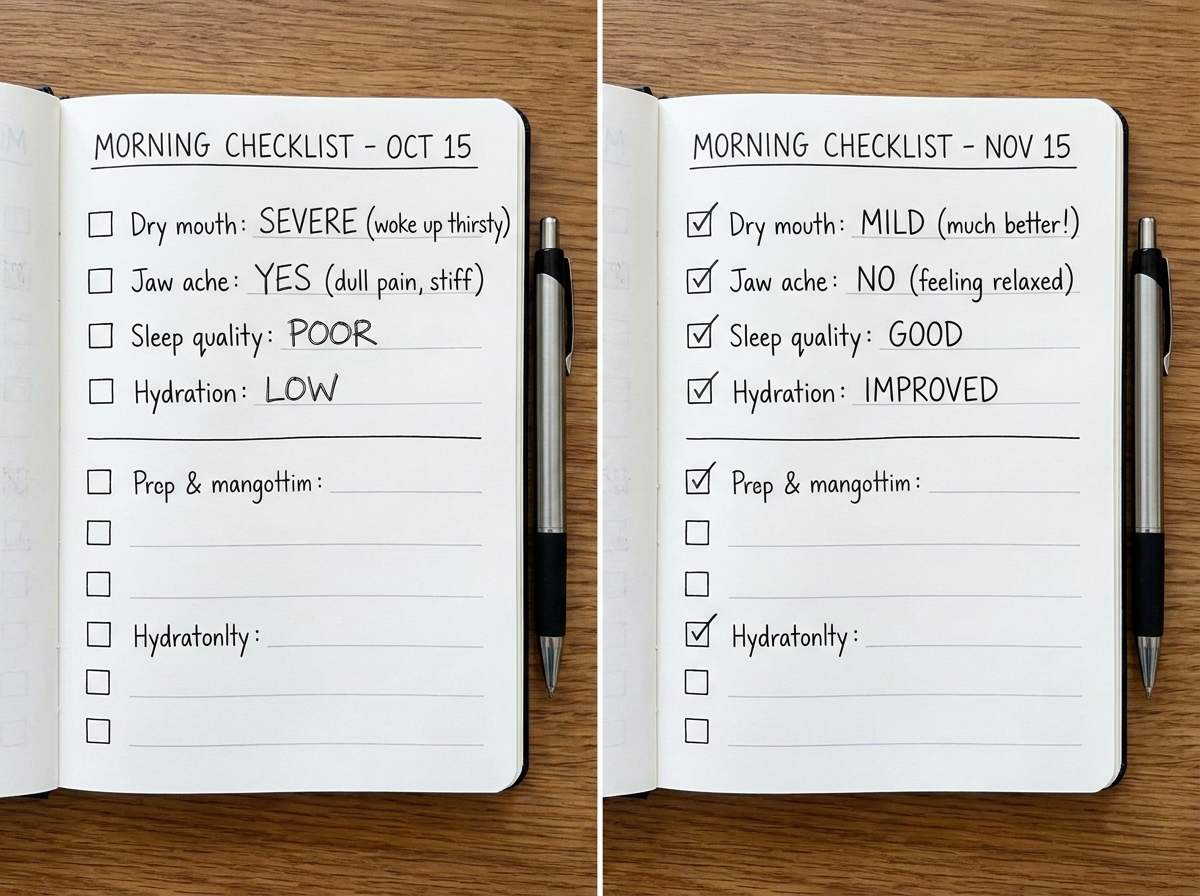
If you’ve ever woken up with a dry mouth, sore jaw, or that “why does my face feel tired even after sleep?” feeling, you already know mouth breathing can hijack your day.
If you’re looking to learn mouth breathing to nasal breathing for sleep and oral health, this is the path that actually changed how my mouth, jaw, and breathing felt day-to-day. The core shift isn’t “willpower to breathe through your nose,” it’s figuring out what’s physically driving the pattern—tongue posture, lip seal, nasal airflow habits, and how your sleep-disordered breathing shows up in your mouth. Once I started treating breathing like a system (not an isolated habit), my oral discomfort stopped being random.
- You need to spot why your mouth is open (airflow, tongue posture, friction), not just close lips.
- Expect a phase where sleep feels worse before it stabilizes as tissues and patterns recalibrate.
- Your best feedback loop is morning symptoms plus jaw/neck tension, not how “motivated” you feel.
Definition: What “mouth breathing to nasal breathing” means for you
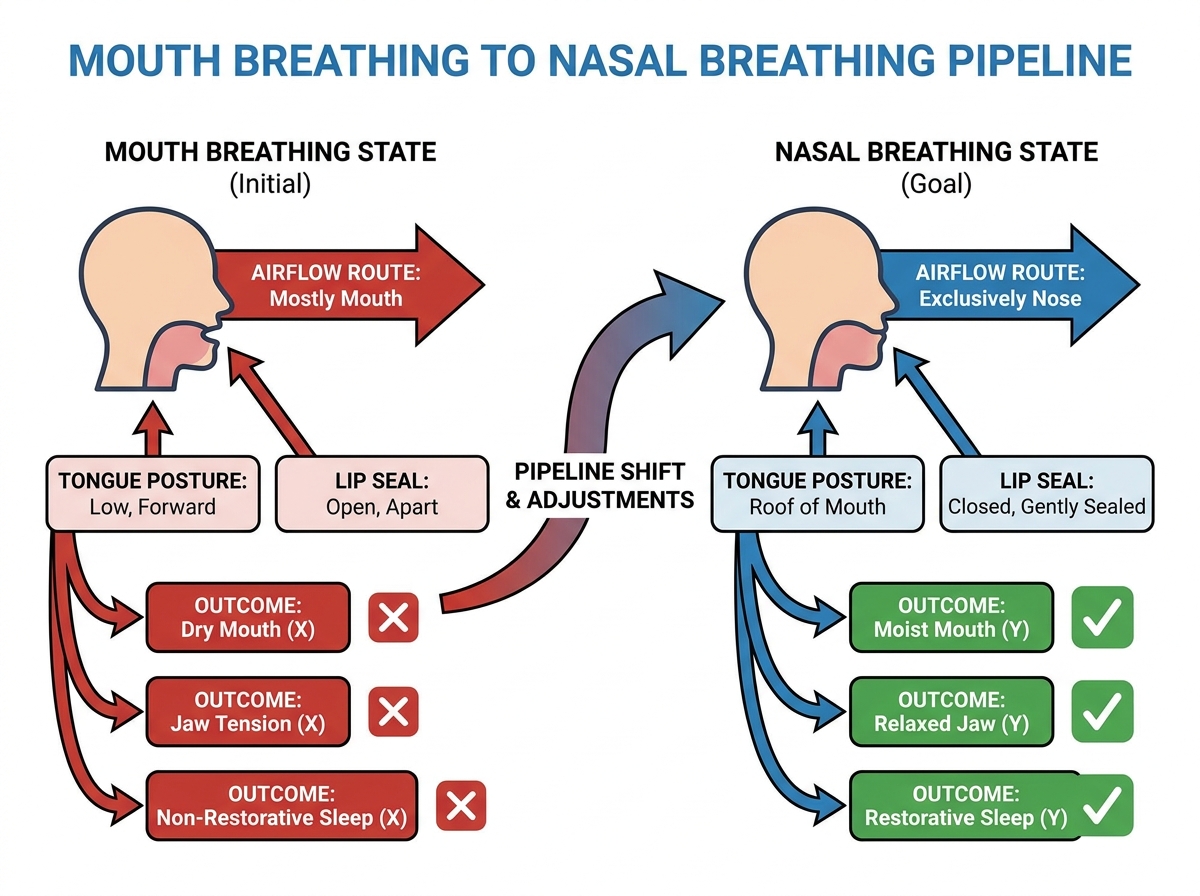
Mouth breathing to nasal breathing means retraining the way air moves through your nose during the day and—more importantly—while you sleep, so your lips, tongue, and jaw stop compensating for poor airflow. For me, the difference became obvious when I stopped treating my mouth like the problem and started treating my breathing route as the cause.
Two patterns matter most: mouth opening during the day (often linked to tongue posture and facial muscle tension) and sleep-disordered breathing (snoring, unrested sleep, dry mouth). If you’re trying to improve oral health, you’re really trying to reduce the mouth-drying cycle that inflames tissue and can worsen jaw discomfort.
Sharp insights
- Closing your lips doesn’t fix the breathing route.
- Dry mouth at night can start as jaw tension.
- Tongue “rest” is a breathing skill, not a posture cue.
How nasal breathing changed my oral pain cycle
The first time I tried “just breathe through your nose,” I felt smug for about ten minutes—then my jaw started protesting. My tongue felt like it was stuck trying to do two jobs at once: maintain a seal while also compensating for airflow. That’s when I realized mouth breathing wasn’t a single habit. It was a strategy my mouth and jaw used to keep me functional.
When I finally slowed down, I started tracking what happened right after I forced nasal breathing. If my mouth dried out faster, my jaw clamped, or my throat felt tight, I knew I was pushing past the bottleneck instead of clearing it. That’s the moment I stopped thinking in “good vs bad breathing” and started thinking in “what’s limiting me right now?”
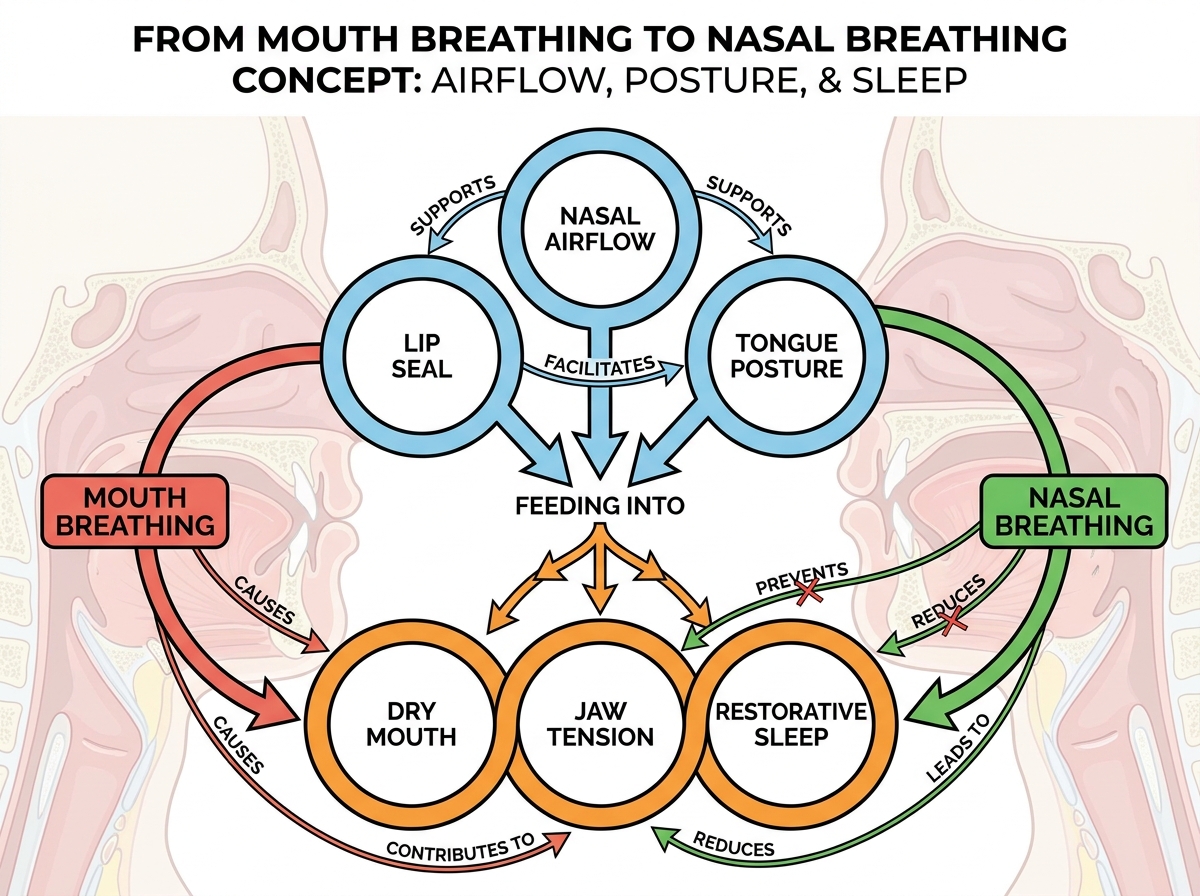
The breakthrough wasn’t a secret exercise—it was recognizing the chain reaction. Once nasal airflow improved even slightly, my mouth stayed less irritated, and my jaw stopped feeling like it had to work overtime to keep my airway stable. My oral discomfort started to behave like something with a cause, not like random flare-ups.
The real reason you end up mouth breathing (and how I caught it)
People make the same mistake I did: they blame the easiest visible behavior. If my lips were apart, I assumed the solution was lip closure. If my tongue looked “low,” I assumed the solution was to shove it up. But the deeper pattern was that my body kept choosing mouth opening when my nose couldn’t deliver comfortably.
In my own self-checks, I learned to watch for friction cues—things like how quickly I got irritated at the nostrils when I tried to nasal breathe, or how my throat felt as I shifted airflow. Sometimes my mouth opened because of airflow discomfort. Sometimes it opened because my jaw posture made it harder to breathe quietly.
Once I started doing that diagnosis instead of guessing, my training became simpler. I didn’t jump straight into endurance. I worked in tiny transitions—learning to keep airflow stable while my tongue and jaw settled. That reduced the “rebound” where I’d feel better during the day but worse at night.
And that’s why mouth breathing to nasal breathing for sleep and oral health isn’t about being perfect. It’s about removing the triggers that force your body back to the mouth as the default.
Breathing re-education: the moment it finally felt doable
Breathing re-education sounds so clinical that I expected it to feel hard. Instead, mine became practical once I stopped treating it like a performance and started treating it like calibration. The first few days felt awkward because my mouth kept trying to win. My throat would tense, my jaw would brace, and I’d catch myself swallowing like I was “resetting” a system.
The mistake I almost made was overdoing the training window. I thought longer sessions would speed things up. What actually happened is that I got fatigued, my tissues got more sensitive, and my breathing felt less stable. When I reduced intensity and focused on transitions, I stopped turning practice into a trigger.
What clicked for me was using a consistent feedback moment: the second I noticed lip separation or jaw clamping, I stopped and adjusted rather than pushing through. It felt like steering, not forcing.
What “frenum assessment” taught me about pain
I didn’t expect anatomy checks to matter, but they did—because they made my pain patterns make sense. When I looked closer at how my mouth tissues moved, I noticed restrictions that changed the way I could rest my tongue and lips comfortably. That didn’t just affect comfort. It changed how breathing mechanics played out inside my mouth.
The lived frustration was this: I’d try to reduce oral pain, but it kept returning in the same places, almost predictably. After I paid attention to movement limits, I stopped treating the pain like a standalone problem. I started treating it like a “how your system is constrained” message.
Once I understood those constraints, my approach changed. I stopped trying to muscle through. Instead, I supported the environment where better breathing could happen—tongue function, oral positioning, and how my jaw needed to move to stay calm.
If you’re dealing with orofacial myofunctional disorders, that shift matters because your body won’t cooperate with nasal breathing if it can’t move smoothly.
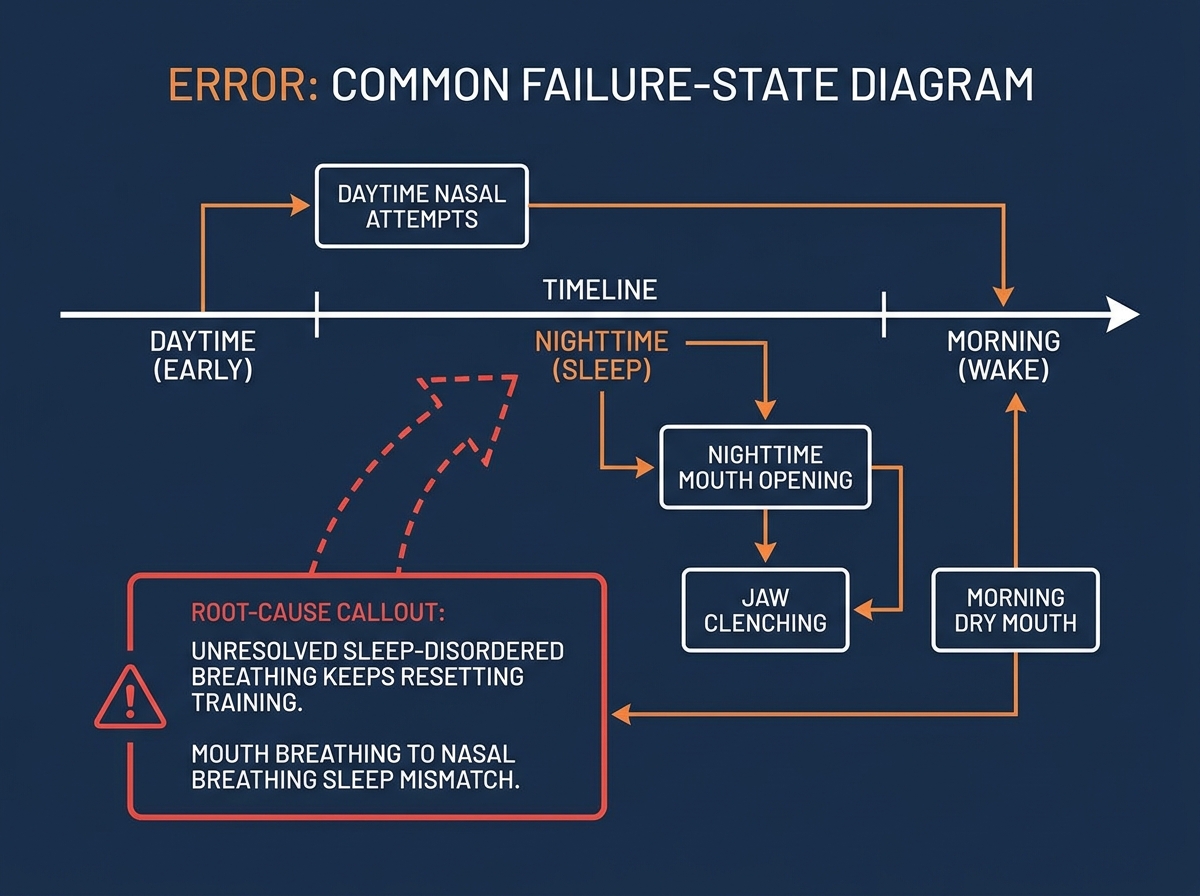
Sleep-disordered breathing: the part I ignored too long
The biggest mistake people make when learning this topic—speaking from my own experience—is assuming snoring, dry mouth, or unrested sleep will “sort itself out” once you train daytime nasal breathing. I trained during the day, felt okay for a few hours, then woke up worse with a dry mouth and that tight jaw feeling.
That taught me that sleep-disordered breathing has its own timeline. If your airway collapses or narrows during sleep, your mouth becomes the backup route. Then oral tissues pay the price overnight, and your jaw starts guarding again.
When I started screening my patterns—especially noticing whether the dry mouth matched other symptoms like snoring or waking up tense—I could connect the dots. My oral health improvements didn’t show up consistently until I treated sleep as part of the same breathing system.
This is where practical oral health promotion stopped being “brush and hope” and became “reduce the mouth-drying cycle while improving airway stability.”
Orofacial myofunctional disorders and why nutrition suddenly mattered
After I connected breathing and sleep to oral discomfort, nutrition felt like a strange add-on—until I realized what it was actually doing. My body’s inflammation tolerance, saliva dynamics, and tissue sensitivity changed based on what I gave it. And when you’re retraining breathing, your mouth tissues can’t just “endure” irritation.
The confusion I had was thinking nutrition would work alone. It doesn’t. It supports everything else. But when I tightened up what aggravated my oral environment, my training became easier. My tongue felt less reactive, my jaw clenching decreased, and the rebound into mouth breathing felt less automatic.
If you’re trying to understand nutrition and OMDs, my experience is that the best results came from pairing food choices with the mechanical work: tongue function, lip seal, and sleep airway stability. That combination is what made changes stick.
If you’re also balancing broader health habits, you may like this perspective on deep skill acquisition and outcomes: How to Learn a Skill Deeply: A Real-World Journey.
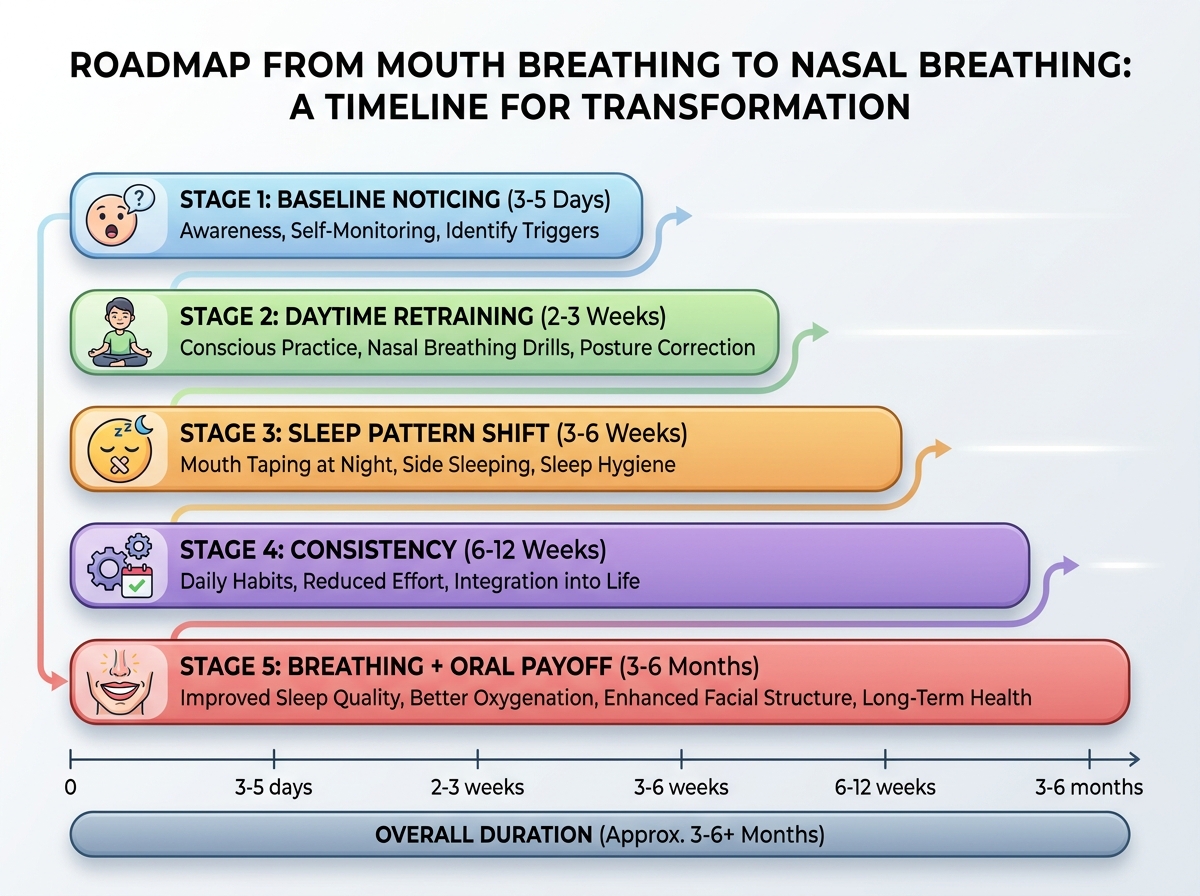
Sleep and oral health timeline: how long does it take?
| Stage | Content | Time |
|---|---|---|
| Baseline noticing | Track morning dry mouth, jaw tightness, and nighttime patterns | 3–5 days |
| Daytime retraining | Build nasal airflow transitions, calm tongue/jaw posture | 2–3 weeks |
| Sleep pattern shift | Reduce mouth opening at night, watch for dryness rebound | 3–6 weeks |
| Consistency | Symptoms stabilize; oral comfort becomes less “spiky” | 6–12 weeks |
| Breathing + oral payoff | Better morning oral comfort, fewer flare-ups, steadier rest | 3–6 months |
| Total estimated time | Combined retraining and stabilization window | 3–6 months |
Order matters more than speed. Being slower than the estimate can still mean you’re doing the right work.
Oral health promotion that actually matches what my body needed
Once I connected breathing to oral health promotion, I stopped treating daily care like separate boxes. I focused on keeping my mouth environment stable—especially at night—because that’s when my pattern used to undo all my effort.
I became more specific with what I targeted. Instead of generic “be careful with your teeth,” I worked on reducing mouth dryness, easing my jaw guard response, and supporting tongue function so my oral tissues stayed comfortable enough to cooperate with nasal breathing.
What felt different after a while is that my oral comfort started responding to changes I could feel: a calmer jaw, steadier breathing, less irritation. That’s when it stopped feeling like I was learning a concept and started feeling like I was managing a system.
Disease prevention and management: what I’d do first now
When I finally look back at the path that helped most, it’s not the most complicated technique. It’s the sequencing. I would start with airway-breathing reality, then address oral muscle patterns, and only then lock in long-term prevention habits.
That order reduced my risk because it removed the drivers of tissue irritation. Mouth breathing kept my mouth dry, and dry mouth changes the whole oral ecosystem. Once that cycle weakened, disease prevention felt less like chasing symptoms.
If you’re a practitioner or a wellness-focused person integrating this into care, the biggest shift is mindset: you’re not just managing oral discomfort. You’re managing how breathing, sleep, and orofacial mechanics interact.
Practical application: what worked in real situations for me
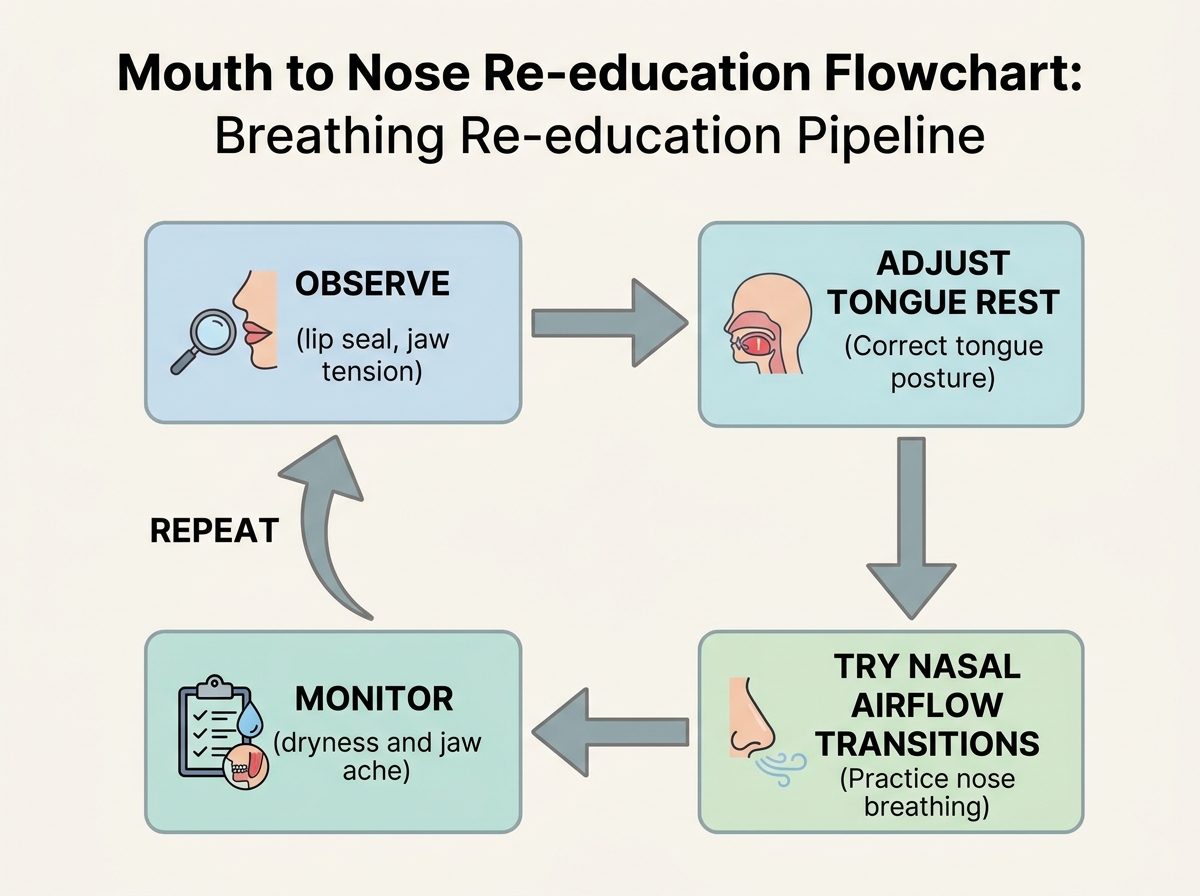
Case study mode helped me stop “performing” knowledge. I’d start by observing what my mouth was doing—lip position, jaw tension, and the way my tongue tried to find a stable rest. Then I’d test small changes that affected airflow and comfort rather than chasing perfection.
The moment I started using that kind of structured observation, my progress improved because I stopped relying on memory. I could see which adjustments increased comfort and which ones triggered relapse into mouth opening.
Even in tougher moments—when my sleep felt off or my jaw felt sensitive—I didn’t treat it like failure. I treated it like data. That’s what made the whole journey feel human instead of theoretical.
Closing
Looking back, I’m surprised by how much of my “oral health problem” was actually a breathing and sleep problem wearing an oral disguise. Once I stopped fighting the pattern and started working with it, nasal breathing became less like a demand and more like a new default my mouth could support.
Track morning symptoms, not just daytime comfort. Your mouth often tells the truth when you first wake up.
Use shorter nasal attempts with faster resets. Overtraining made my tissues more reactive and pushed me back to mouth opening.
Adjust tongue and jaw together, not separately. A “good tongue” without jaw calm still breaks airflow stability.
Treat snoring and dry mouth as the same system signal. If sleep-disordered breathing remains, daytime wins won’t hold.
Recheck for movement restrictions when pain repeats. Myofunctional patterns can keep returning through the same mechanical bottleneck.
Support tissue comfort with nutrition, then mechanical work. Food choices helped my mouth cooperate with the breathing changes I was making.
Document what triggers mouth opening during transitions. The relapse pattern usually points straight to the real friction point.
Keep prevention tied to airway habits. When dryness drops, oral disease risk management becomes dramatically easier.
Leave a Reply