I kept trying to “train harder” the way I would for other clients, and Parkinson’s kept punishing me for it—through fear, missed sessions, and unsteady progress.
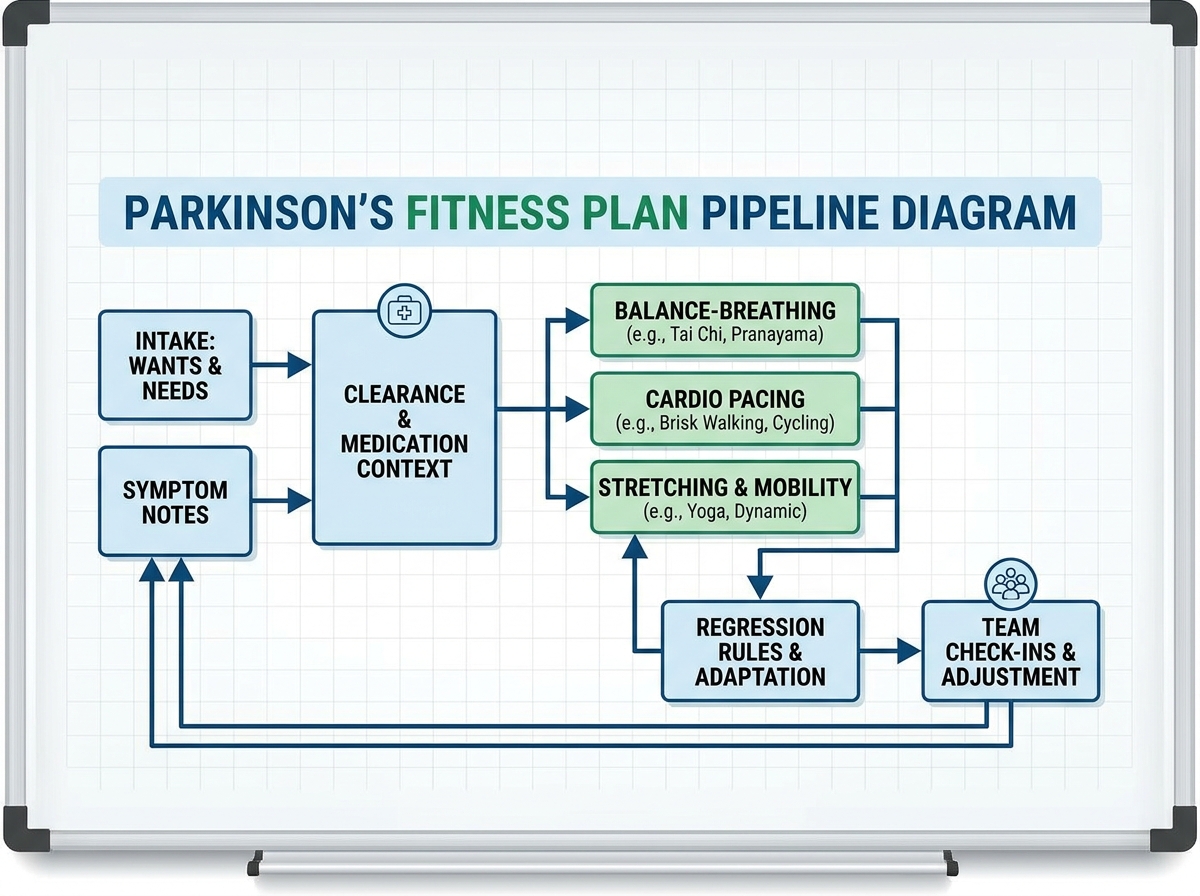
If you’re looking to learn Parkinson’s fitness plan, start by building a program around what the person wants to avoid, what their symptoms are doing today, and what their body can safely handle with medication in mind. The biggest shift for me was treating exercise like a coordinated medical conversation, not a gym routine—so I planned the warm-up, balance work, and cardio with clearance, context, and clear stop points. Once I stopped improvising and started running a consistent client-focused line of defense, everything got simpler: decisions felt safer, and adherence went up.
- Start with symptom-aware wants and needs, then design around clearance and medication reality.
- Use balance-first progressions, cardio with intention, and stretching that targets real stiffness.
- Keep the team loop tight—doctor, caregiver, and you—so regressions don’t blindside you.
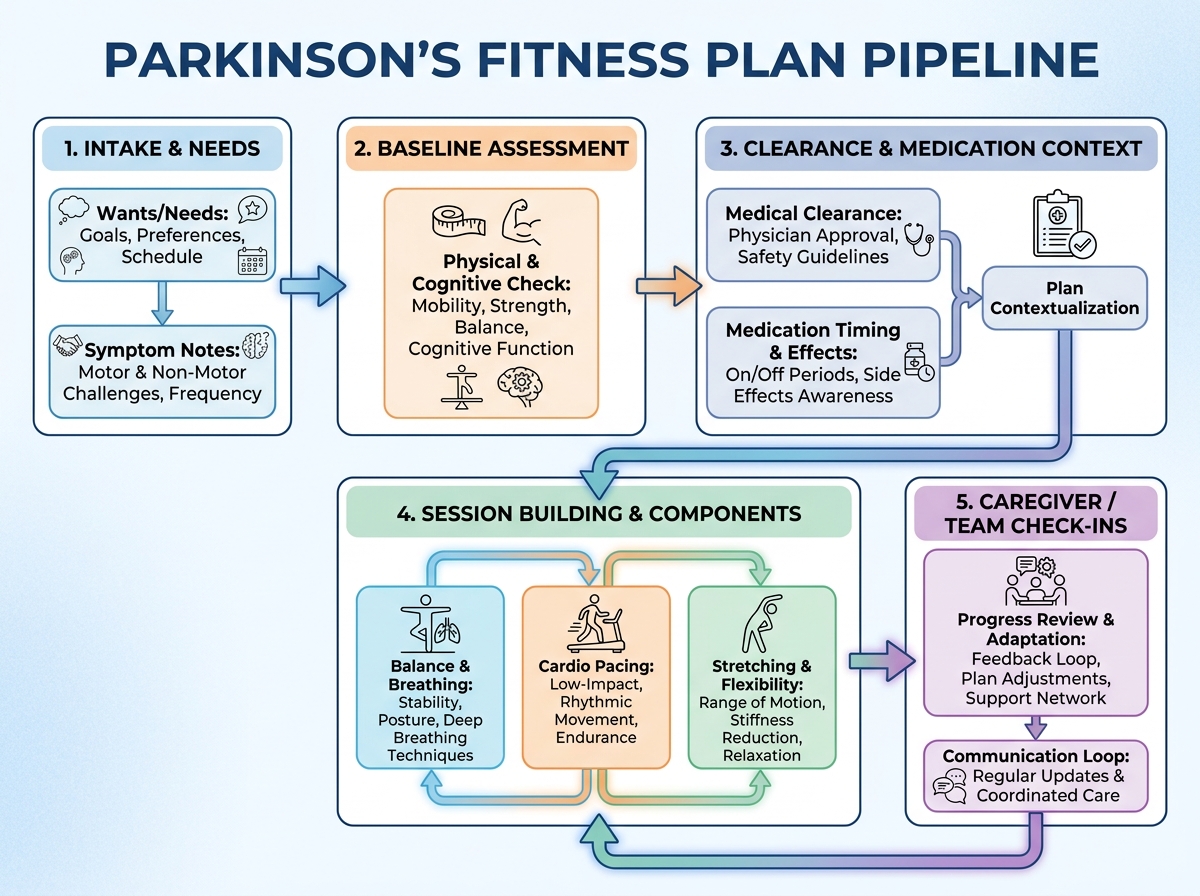
If you’re asking, “What is a Parkinson’s fitness plan?” it’s a structured exercise approach built for someone whose movement system changes over time. The plan uses symptom patterns (balance, breathing, cardio tolerance, stiffness, focus) to pick exercises, dosing, and progressions. For safety, it also works inside medical constraints by knowing what to avoid and when to pause.
Here’s the simplest way to distinguish the common types I had to separate in my own work:
- Balance and breathing focus: short sessions that train stability under real daily conditions.
- Cardio with pacing logic: intensity that supports function without triggering wipeouts.
- Mobility and stretching: targeted range work that matches how the body tightens during the day.
- Caregiver-supported structure: routines that survive real-life interruptions.
It’s not just “exercise for Parkinson’s.” It’s exercise with constraints, context, and communication.
People try to “fix everything” in one week and burnout.
You can’t progress without a clear definition of “regression.”
Balance training is more about decisions than reps.
| Stage | Content | Time |
|---|---|---|
| First setup | Clarify wants/needs, baseline info, and safety boundaries | 1–2 days |
| Initial assessment | Track symptoms, breathing, balance, and daily constraints | 2–4 sessions |
| Build the routine | Choose cardio, stretching, regression rules, and session structure | 1–3 days |
| Start small | Run a first week with journal check-ins and caregiver input | 1 week |
| Adjust and lock in | Tighten progressions, refine “what to avoid,” reduce variance | 2–3 weeks |
| Total estimated time | Enough to run a working Parkinson’s fitness plan safely | ~4–6 weeks |
Order matters more than speed, especially when balance and medications complicate the day. If you move slower, you’re usually building something that can actually last.
The first thing I stopped doing
When I first started working with people who have Parkinson’s, my default was to treat training like a neutral container: you pick movements, you add sets, and “improvement” follows. That sounds logical until the person’s day is shaped by symptoms that change hour to hour. I remember thinking the program was fine—until a session left someone shaky in a way they didn’t recover from quickly.
The moment things clicked was realizing the “starting point” isn’t their diagnosis. It’s their wants and needs, what they’re trying to avoid, and what their symptoms are actively doing right now. I stopped asking only, “What exercise do you need?” and started asking, “What do you not want your body to do today?”
That changed my planning. If someone wanted to avoid getting worse with walking, I built the early work around stability and breathing before I touched anything that felt like “conditioning.” If they were most frustrated by stiffness, stretching became a non-negotiable part of the session instead of an add-on.
I also learned that their past matters more than my assumptions. Whether they’d worked with a trainer before or struggled with routines in the past tells me how likely they are to stick with something that feels safe—not just something that looks impressive.
How I turned “symptoms” into a plan
I made the same mistake a lot of beginners make: I wrote workouts based on the broad category of Parkinson’s instead of the specific pattern happening in front of me. The breakthrough came when I started treating assessment as ongoing, not a one-time checklist. Each week, I reviewed what the person could do, what they avoided because of fear, and what changed after medication.
Baseline info for Parkinson’s isn’t just “can they balance?” It’s also how they breathe, how they transition (sit-to-stand, turn, step), and whether focus breaks down when effort rises. I got more honest about mental fatigue and clarity, because I saw sessions fail when people tried to muscle through without the cognitive support their body needed.
When I finally designed around balance and breathing early, it felt like the program stopped fighting them. They weren’t “just exercising”—they were learning how to control their movement and their breath during the parts of the day that usually feel unpredictable.
This is where longtail variants started to stop sounding like buzzwords: “balance and breathing” became the anchor for how I structure a Parkinson’s session when everything else is up in the air.
Cardio that didn’t wreck the day
Cardio is where I used to overreach. I’d pick a treadmill plan or a time-based target and hope the body would adapt the way it does in other training contexts. With Parkinson’s, that hope is expensive—because the wrong intensity or timing can trigger a bad day that makes the next session harder.
Once I stopped thinking of cardio as “make them sweat,” I started thinking of it as “teach the body to move reliably under effort.” I asked: can they maintain stability and breathing while working? Can they recover without getting worse? And most importantly, does the plan match what they’re willing to do consistently?
That’s how cardio became less intimidating. I focused on pacing logic, not heroic intervals. I used check-ins tied to how they felt after medication and how their balance looked during and after the work, not just what the machine displayed.
By the time I could name the difference between a cardio block that builds confidence versus one that plants fear, I finally understood why some people stop showing up. The goal wasn’t “more cardio.” It was cardio that supported the rest of their week.
Stretching that targets the real stiffness
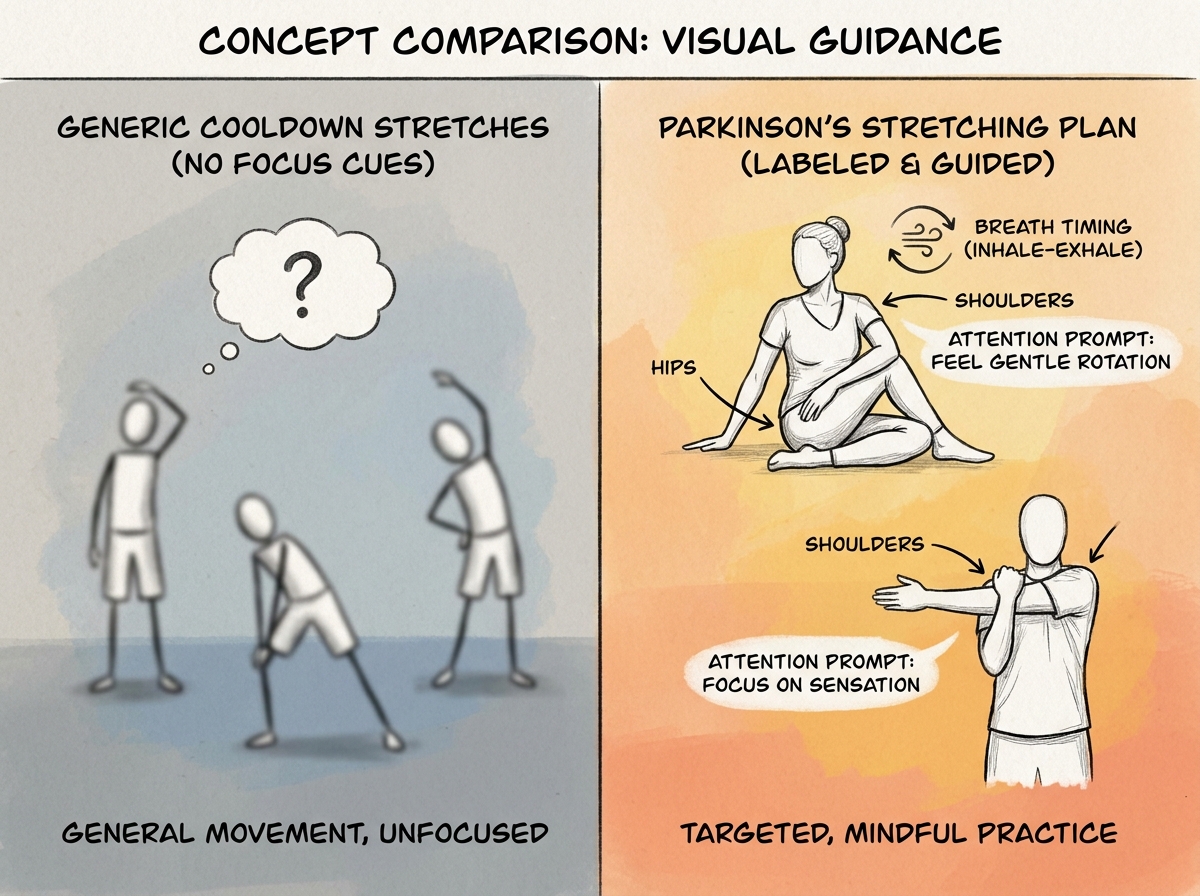
Stretching felt harmless to me—until I saw it fail. I used to treat it like a generic cooldown, but stiffness in Parkinson’s often shows up with specific patterns: shoulders that hold tension, hips that feel locked, and legs that don’t open when you ask them to.
The shift was learning to make stretching part of the plan for what the person experiences between sessions. I designed stretching around daily constraints: when they feel tight, what movements are hardest, and how they move when they’re not fresh. That’s why “Parkinson’s stretching plan” became a phrase I actually cared about, because it forced me to match mobility work to real movement limits.
I also stopped relying on passive-only approaches. I blended stretching with mindful attention—helping the person notice where their body resists and where it finally yields. Even the simplest range work improved when it had clarity and intention instead of being “do this because it’s good for you.”
This is also where mental exercises and focus quietly mattered. If someone couldn’t stay present for the stretch, they weren’t getting the neuromuscular benefit I needed them to get. Their brain had to participate, not just their joints.
Regression rules saved my sessions
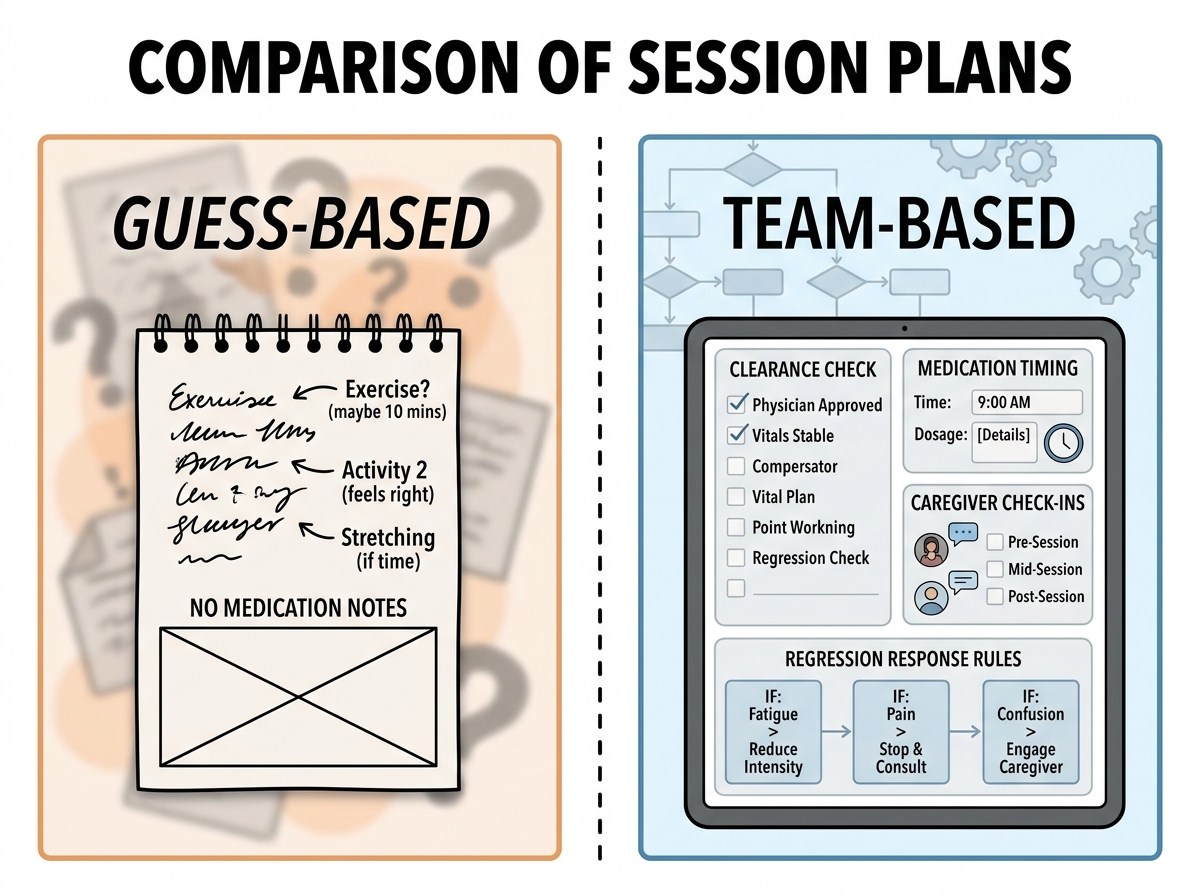
The biggest mistake people make when learning a Parkinson’s fitness plan is assuming regression is random. In my early months, I treated a bad week like a one-off and pushed forward as usual. That felt respectful, until it backfired: the plan stopped feeling safe, and the person started avoiding sessions.
Regression only became manageable when I built rules into how I respond. I defined what counts as regression (not just “they’re tired,” but what changed in balance, breathing, or movement quality), then I created a smaller “same direction” response. Instead of scrapping everything, I reduced complexity first—then intensity—then duration.
That’s when I stopped fighting the body and started guiding it. I used routines that included check-ins and a journal so I could see patterns rather than reacting to emotions. The caregiver part mattered here too, because caregivers notice changes in the day that a trainer might miss if they only see the person during training.
Regression made my plan smarter. Instead of pretending every session will be good, I designed for the reality that some days require adjustment.
Building communication like it’s part of training
Once the exercise got more specific, communication became the real differentiator. I used to think the “team” was for emergencies. Then I watched how well things ran when we communicated often—before problems turned into crises.
I learned to speak in practical terms to doctors and physical therapists. Not just symptoms in general, but what I saw in sessions: balance under effort, breathing quality, transitions, and whether certain exercises looked like they increased risk. The point wasn’t to argue with medical decisions. The point was to reduce guesswork and keep safety at the center.
Caregivers turned out to be the missing piece I didn’t realize I had. When caregivers helped reinforce the plan at home, the routines stopped collapsing under real life. That meant medication timing and daily constraints became part of the training reality, not a footnote.
This also reshaped how I used AI tools in the workflow—not as a replacement for clinical thinking, but as a way to organize questions, keep a journal, and produce consistent prompts for check-ins. When I used it to help me stay clear and structured, it lowered my mental load. When I used it to “decide,” I got reckless.
If you’re working with a client’s Parkinson’s journey, your communication rhythm is the plan.
Putting it all together without losing yourself
The strangest part of mastering Parkinson’s fitness wasn’t learning new exercises. It was learning to hold structure in the middle of uncertainty. I had to stop treating every week as a fresh reset. Instead, I treated progress like a negotiation between the body, the day, and the team.
My routine evolved into something repeatable: baseline awareness, balance and breathing first, cardio with pacing logic, stretching that matches real stiffness, and regression rules that protect momentum. When focus and clarity dipped, I adjusted complexity. When fear showed up, I made safety visible through consistency.
By the time I could run the whole Parkinson’s fitness plan cycle smoothly, I looked back and realized the plan didn’t work because it was “perfect.” It worked because it was specific enough to keep decisions simple and flexible enough to handle the inevitable bad days.
For anyone trying to help Parkinson’s patients, the biggest win is building a system that you can execute even when you’re tired, overwhelmed, or unsure.
10 things you can do immediately
Write “wants and needs” as today’s checklist. This prevents you from designing around a diagnosis instead of the person’s reality.
Do balance and breathing first, every time. It stabilizes the session and reduces the chance of confusion later.
Turn cardio into a pacing question, not a time goal. You’ll protect recovery and avoid wipeout-style setbacks.
Build stretching around the joints that actually lock up. Generic cooldown stretching often misses the stiffness pattern that matters.
Define regression before you need it. When things go wrong, you’ll respond with rules instead of panic.
Use check-ins tied to how the person feels after medication. Medication context changes the meaning of “good” and “bad” sessions.
Include the caregiver in the loop early. They can confirm day-to-day changes that trainers never see.
Keep a simple journal and look for patterns weekly. Consistent notes expose triggers faster than memory does.
Ask the doctor in specific, observable language. You’ll get clearer guidance when you describe balance, breathing, and transitions precisely.
Practice “same direction” adjustments. Reduce what hurts first (complexity, then intensity, then duration) instead of scrapping everything.
If you want one mindset shift that keeps everything coherent: treat the plan like a living line of defense, not a static program.
For more on building skill deeply through real-world constraints, see How to Learn a Skill Deeply: A Real-World Journey Through Mastery.
Leave a Reply