The first time you sit down with a full SPI practice test, the questions don’t feel like physics — they feel like a foreign language written by someone who really wanted to confuse you.
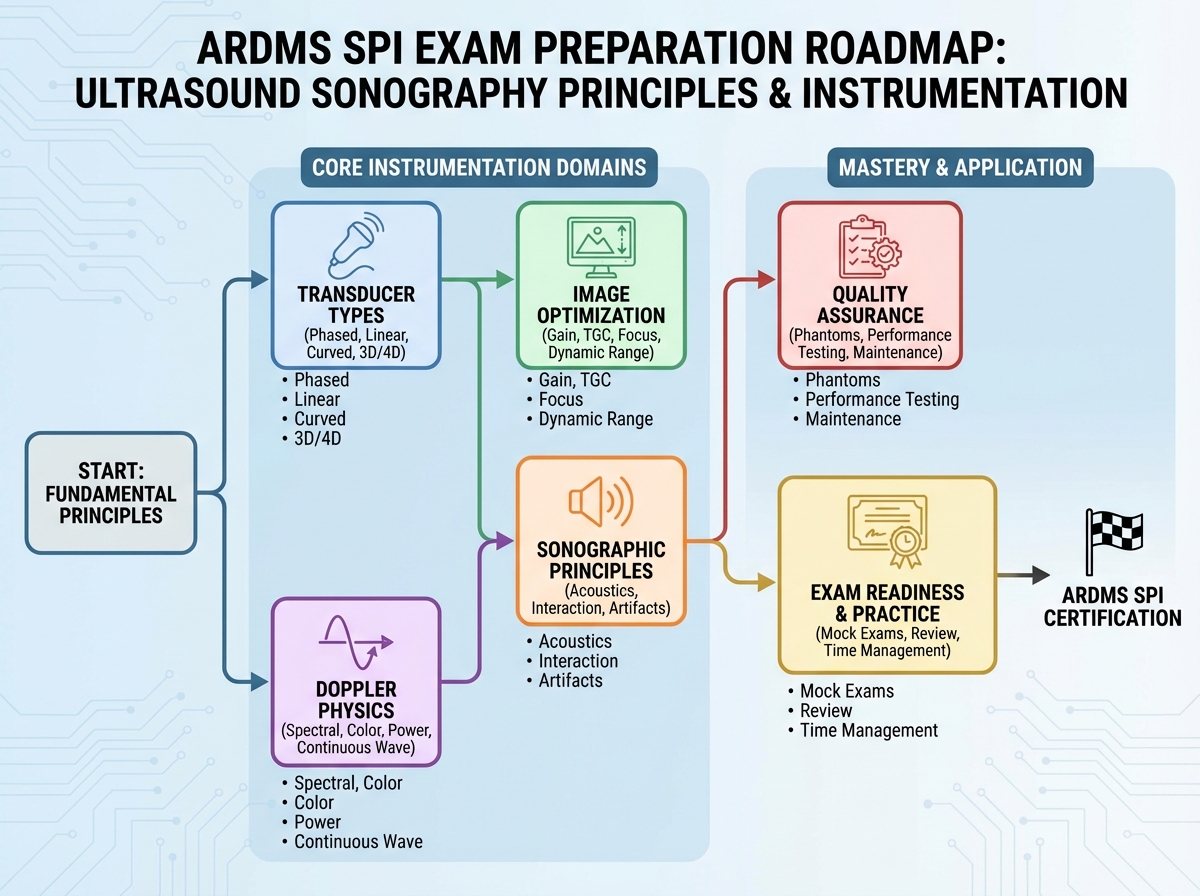
If you’re looking to learn ARDMS SPI exam material the right way, the path isn’t memorizing definitions. It’s building a mental model of how sound actually behaves in tissue — and then layering instrumentation logic on top of that. The SPI is a 110-question, computer-based exam scored on a 300–700 scale, with 555 as the passing threshold. The first-time pass rate sits around 71%, which means nearly one in three candidates fails — not because the content is impossible, but because they studied the wrong things in the wrong order.
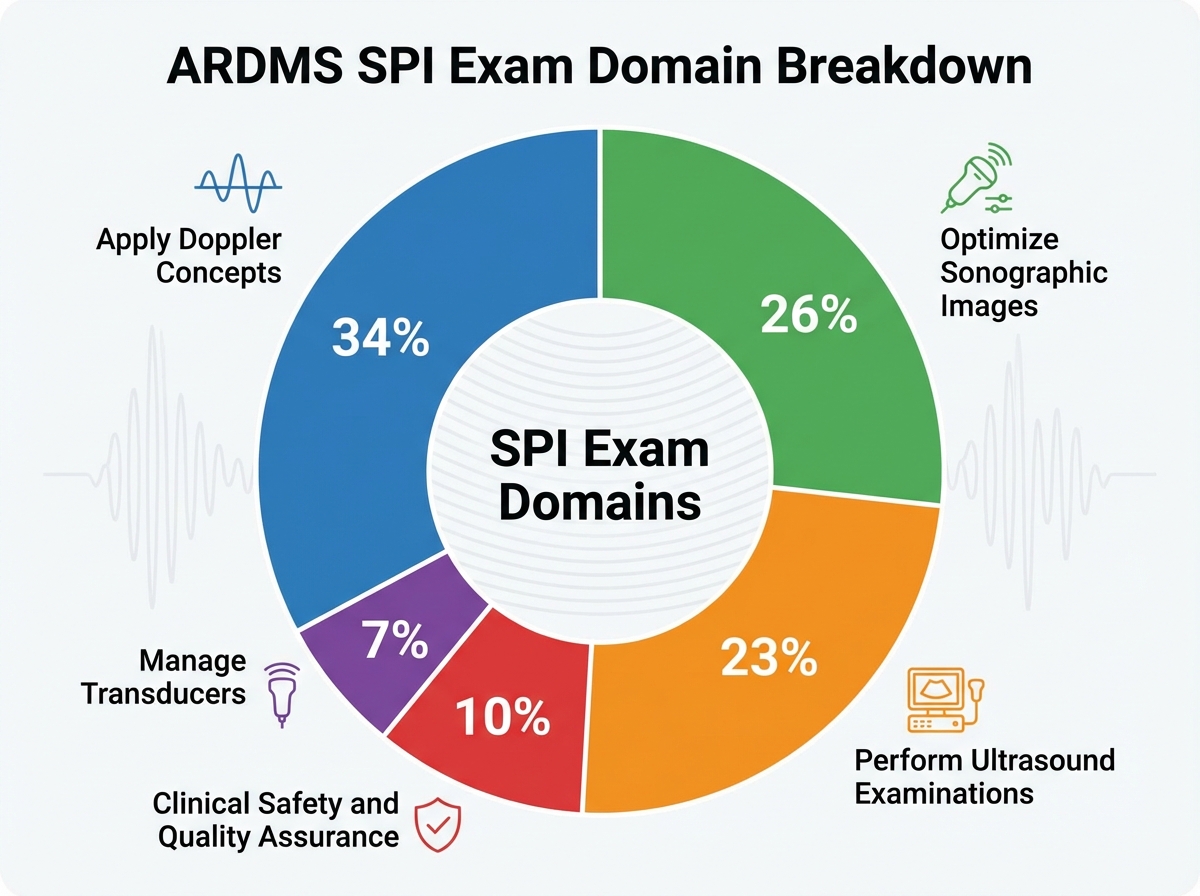
- Doppler concepts make up 34% of the exam — more than any other domain — yet most candidates spend the least time on it
- Passing requires roughly 80–85 correct answers to safely clear the scaled score threshold of 555
- The exam uses clinical scenario framing, so recognizing what’s being asked matters as much as knowing the answer
What the SPI Exam Actually Tests
The SPI — Sonography Principles and Instrumentation — is not a specialty exam. It’s the foundational credential that gates every ARDMS certification: RDMS, RDCS, RVT, and RMSKS. You cannot earn any of those without first passing the SPI. That makes it both unavoidable and oddly underestimated by students who assume it’s “just physics.”
The exam covers five domains. Domain 4 — Applying Doppler Concepts — carries 34% of the exam weight, making it the single biggest determinant of your score. Domain 3 (Optimize Sonographic Images) comes in at 26%, and Domain 1 (Perform Ultrasound Examinations) at 23%. Together, those three domains represent over 80% of your score.
| Domain | Weight | Focus Area |
|---|---|---|
| Perform Ultrasound Examinations | 23% | Physics, pulse-echo, transducer interaction |
| Manage Ultrasound Transducers | 7% | Transducer types, care, selection |
| Optimize Sonographic Images | 26% | Artifacts, resolution, controls |
| Apply Doppler Concepts | 34% | Doppler physics, color/spectral/CW/PW |
| Clinical Safety & Quality Assurance | ~10% | ALARA, bioeffects, QA protocols |
Three things the SPI punishes without mercy:
- Confusing similar-sounding terms (e.g., spatial resolution vs. temporal resolution, or PRF vs. pulse repetition period)
- Knowing the concept but not recognizing it in a clinical scenario wrapper
- Underestimating Doppler — treating it as a minor topic when it owns a third of the exam
The Physics Wall Everyone Hits First
Most people hit the same wall early: ultrasound physics feels abstract in a way that anatomy never did. You can see a kidney on a scan. You cannot see acoustic impedance mismatch. So the brain resists it.
The mistake almost everyone makes when learning SPI material is studying physics terms in isolation — memorizing the formula for the Doppler shift equation without understanding why the angle to flow matters, or what happens to your reading when you exceed 60 degrees. That kind of rote learning gets you through the easy questions and falls apart the moment the question adds a clinical detail.
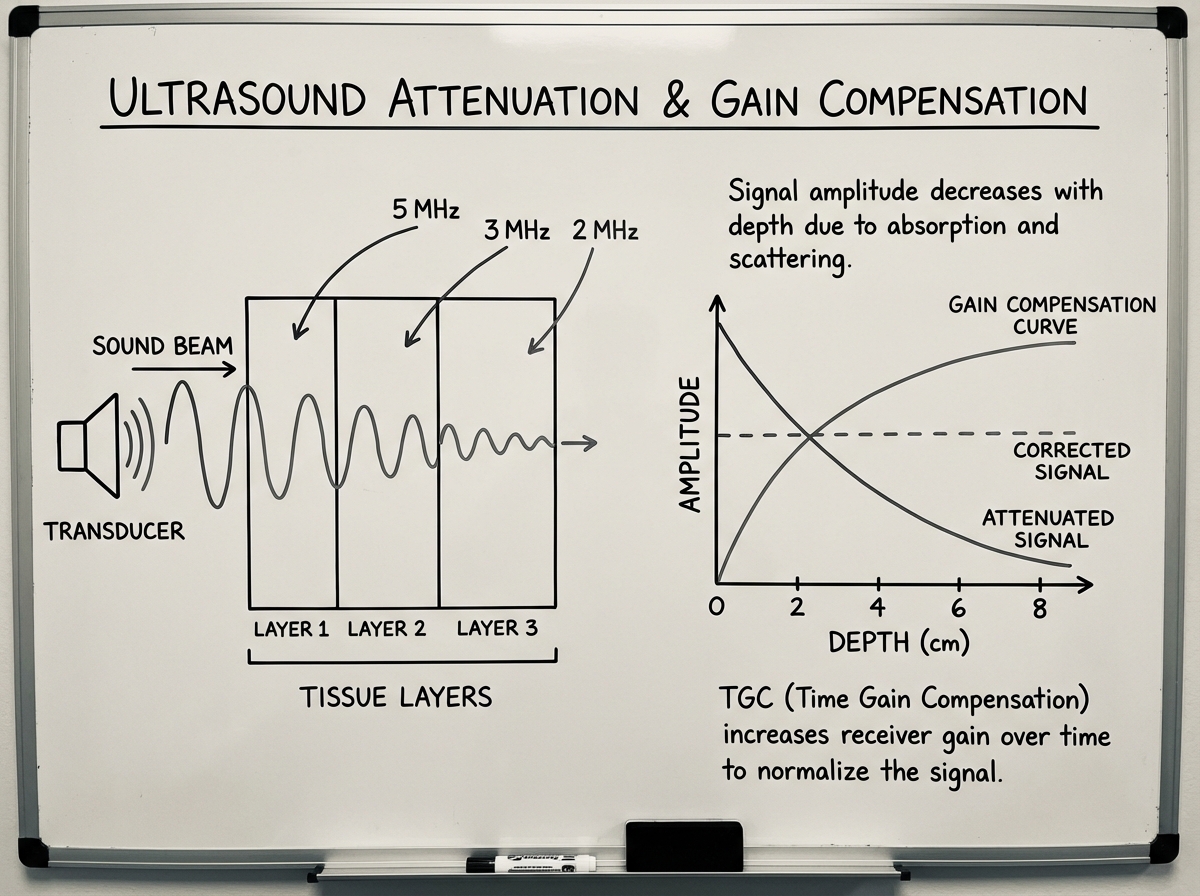
The shift happens when you stop thinking about physics as a set of rules to recall and start thinking about it as a description of what sound is doing inside the body. Attenuation isn’t a vocabulary word — it’s the reason you increase gain when imaging deeper structures. Acoustic impedance mismatch isn’t a formula — it’s why you can see the diaphragm so clearly, and why air makes imaging impossible. Once the physics has a reason, it stops feeling like memorization.
For anyone transitioning into the healthcare field specifically for a sonography career, the foundational principles behind learning computer science with Python and Jupyter Notebooks parallel the SPI in an interesting way — both require building mental models before the surface-level details make sense.
How Doppler Actually Works — and Why It Owns the Exam
Doppler is where the SPI separates prepared candidates from underprepared ones. At 34% of the exam, it’s not a topic you can skim. And it’s also the area where the most conceptual confusion lives.
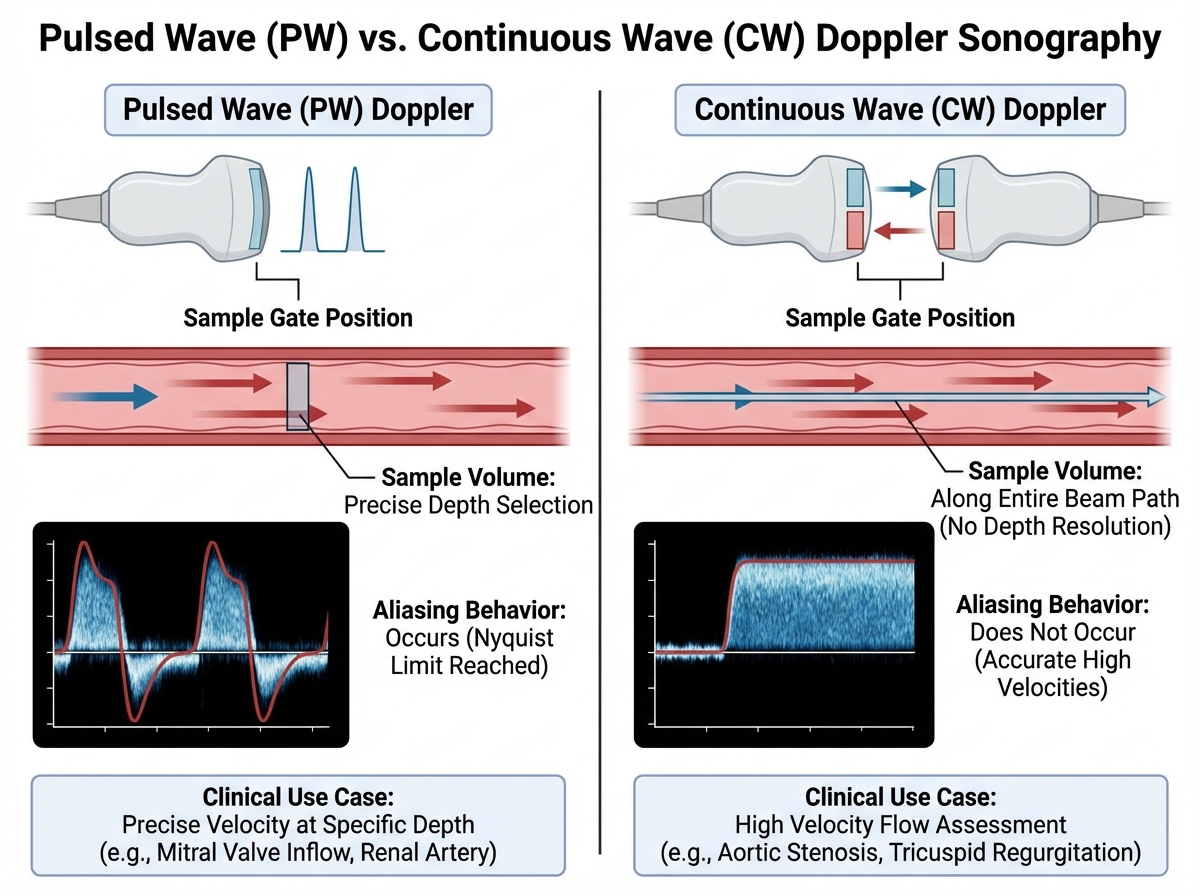
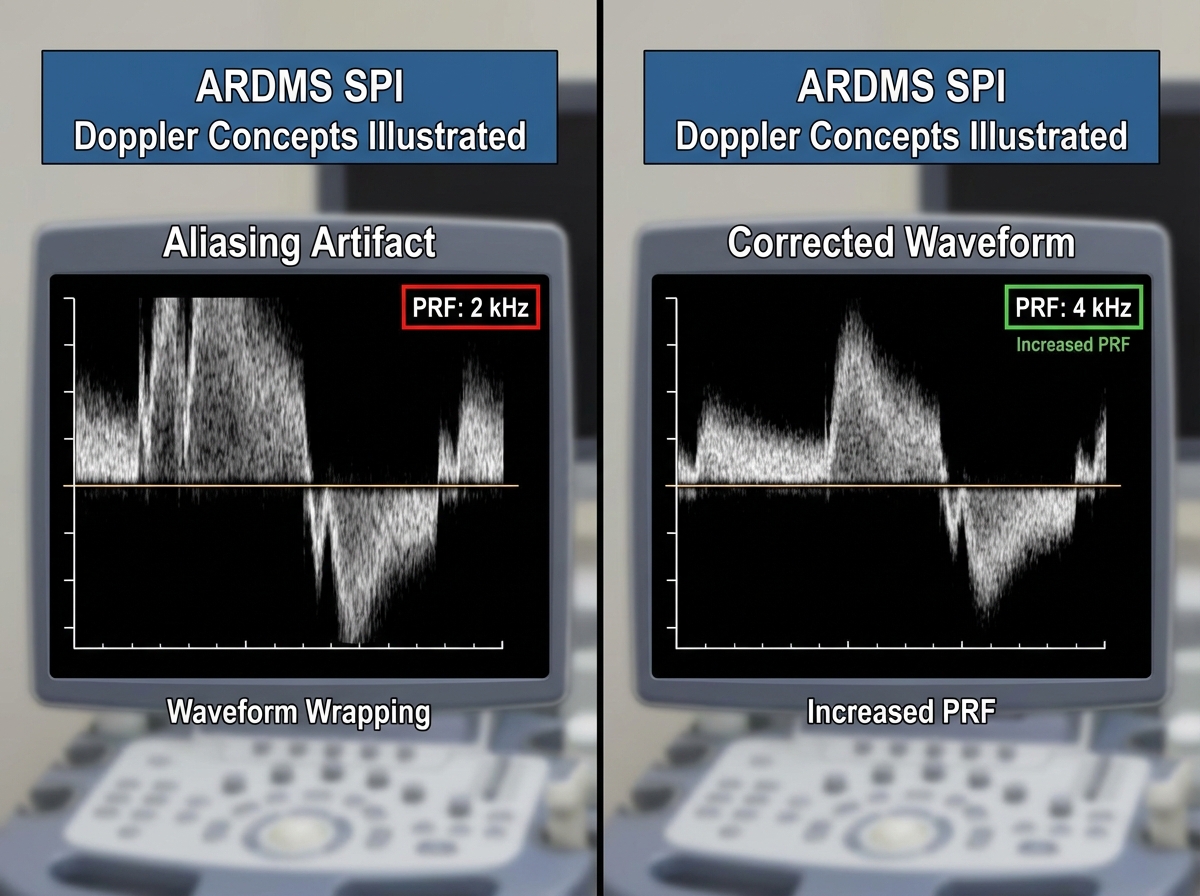
The Doppler effect itself is straightforward: when a sound source and a reflector are moving relative to each other, the received frequency shifts. In clinical ultrasound, the reflector is moving blood. The shift in frequency tells you the velocity of that blood. But the exam doesn’t test whether you understand that sentence — it tests whether you can apply it when the angle changes, when aliasing appears, when you need to choose between pulsed wave and continuous wave, and when color Doppler is being misread because the baseline is set wrong.
Aliasing is the concept that trips the most people. It happens when the Doppler shift frequency exceeds half the pulse repetition frequency — the Nyquist limit. The fix isn’t arbitrary: you either increase the PRF, lower the baseline, use a lower frequency transducer, or switch to continuous wave Doppler. The exam will give you a scenario and ask which adjustment is most appropriate. If you’ve only memorized the definition of aliasing, you’ll pick the wrong answer.
Transducers, Controls, and the Equipment Logic That Connects Everything
Transducer management only accounts for 7% of the exam, but it connects to every other domain. Understanding why you choose a linear array over a curved array, or when a phased array is appropriate, gives context to image optimization questions that would otherwise seem arbitrary.
The image optimization domain (26%) is heavily dependent on understanding what each control actually does to the sound beam. Time gain compensation adjusts for depth-dependent attenuation. Focal zone placement concentrates lateral resolution at the depth you care most about. Dynamic range affects how the machine maps the received echo amplitude to shades of gray. These controls aren’t features to memorize — they’re tools with specific physics justifications. When you understand the justification, the exam question becomes obvious.
One moment that changes everything: when you first understand that the transducer is simultaneously a transmitter and a receiver — and that the machine calculates depth based on the time it takes for the echo to return. That single insight makes pulse-echo imaging, time gain compensation, and depth settings all click into place at once.
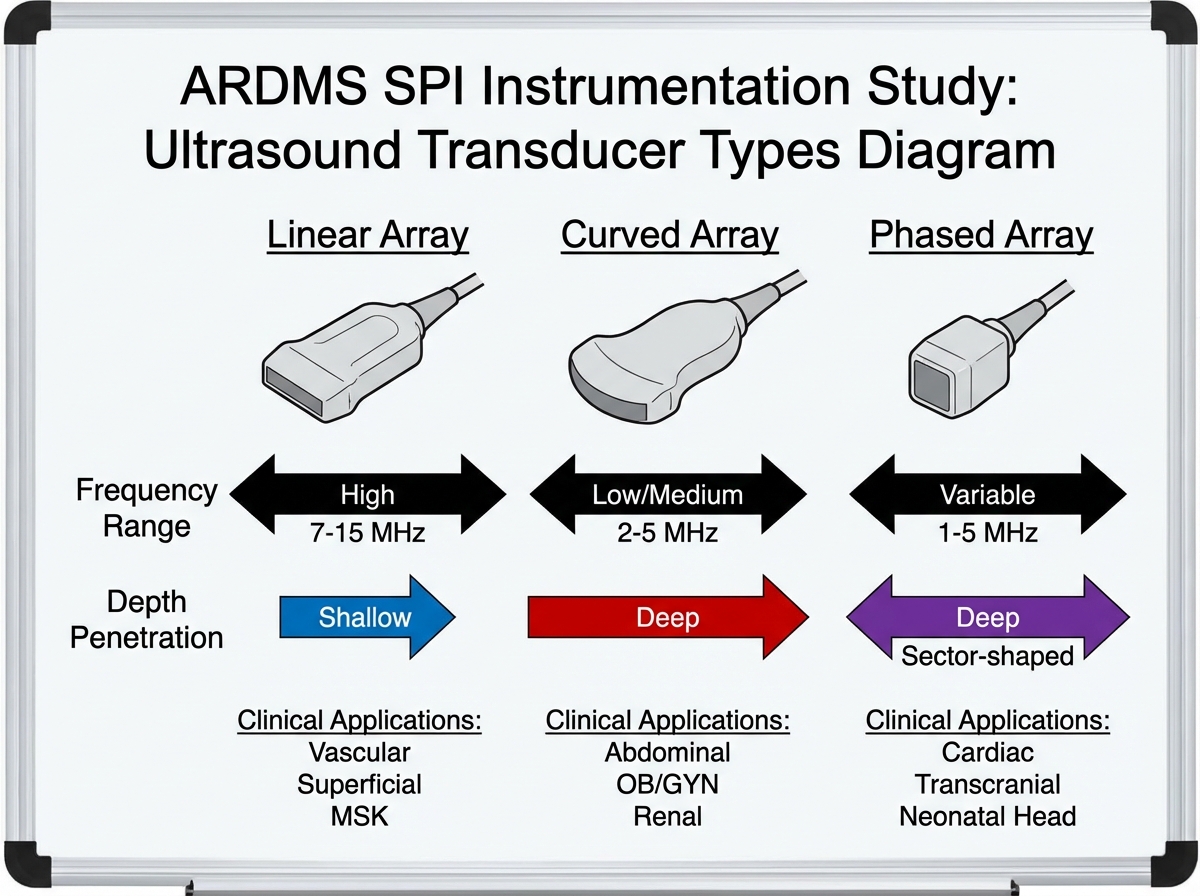
Image Artifacts: The Section That Looks Easy Until It Isn’t
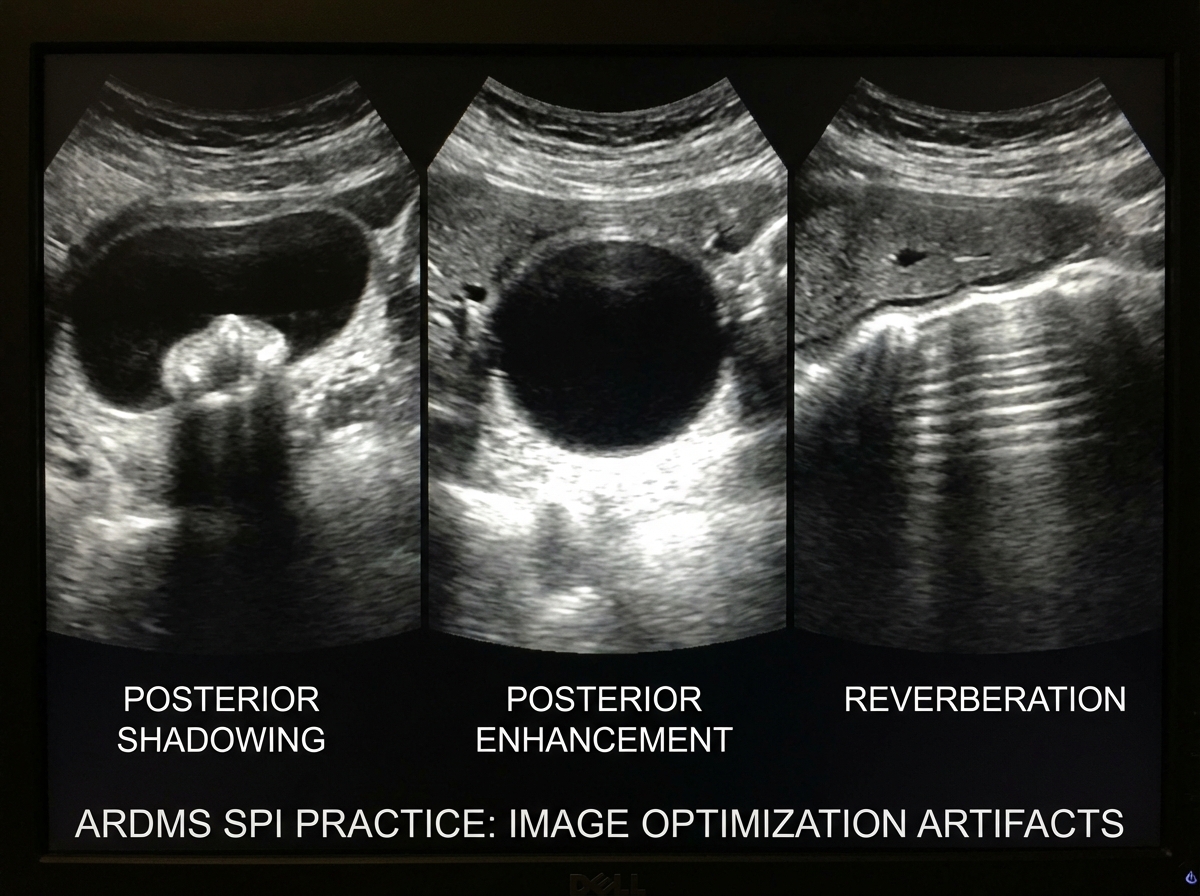
Artifacts sit inside the image optimization domain, and they’re one of the most heavily tested areas in practice exams. The tricky part is that artifacts on the SPI aren’t just identification questions — they’re reasoning questions. “Why does this artifact appear?” and “How would you eliminate it?” are the real format.
The artifacts the exam returns to most often: posterior acoustic shadowing, posterior acoustic enhancement, reverberation, side lobe, mirror artifact, and refraction. Each one has a physical cause tied directly back to how sound interacts with tissue interfaces. Reverberation comes from two highly reflective surfaces creating a repeating echo. Mirror artifact happens when a strong reflector redirects the sound beam. If you traced each artifact back to its physics cause, you’ve essentially studied two domains at once.
The moment things finally clicked for me with artifacts was drawing them. Not reading about them — drawing the actual beam path, the reflector position, and where the machine incorrectly places the echo. That physical diagram made the spatial logic permanent in a way that flash cards never could.
Quality Assurance and Patient Safety: The Domain People Skip
Clinical safety and quality assurance sits at roughly 10% of the exam. It covers ALARA (as low as reasonably achievable), thermal and mechanical indices, biological effects of ultrasound, and QA protocols for equipment maintenance. Most candidates treat this as a light read before the real exam — a few definitions, a few acronyms.
That’s a mistake. The safety questions on the SPI often appear as clinical decision scenarios: “A patient is in the first trimester of pregnancy — which index should you prioritize monitoring?” The answer requires knowing both what thermal index and mechanical index measure and why early pregnancy creates heightened sensitivity to mechanical effects. That’s a two-layer question, not a vocabulary lookup.
Quality assurance questions cover phantom testing, documentation standards, and recognizing equipment malfunction. These feel dry until you realize the exam is testing whether you understand why QA exists — not just what procedures it involves. The “why” is always the exam’s real question.
Practicing Under Pressure: The Study Stage Nobody Talks About
There’s a phase in SPI prep that most people rush past: the transition from studying content to practicing under timed, exam-like conditions. Reading notes builds familiarity. Timed practice under realistic conditions builds the actual skill the exam tests.
The SPI gives you 110 questions in 120 minutes — roughly 65 seconds per question. Some questions take 20 seconds. Doppler calculations can take 2–3 minutes. If you haven’t practiced pacing, you’ll hit the calculation questions late in the exam with three minutes left and a brain that’s already tired.
The most effective practice sequence starts with untimed topic-specific questions to build domain confidence, then moves to mixed-topic timed sets that simulate the real exam randomness. The final two weeks before the exam should include at least two full-length timed sessions reviewed question by question — not just for right answers, but for the reasoning pattern behind each answer choice. Understanding why the wrong answers are wrong is more valuable than confirming why the right answer is right.
How Long It Actually Takes to Be Ready
| Stage | Content | Estimated Time |
|---|---|---|
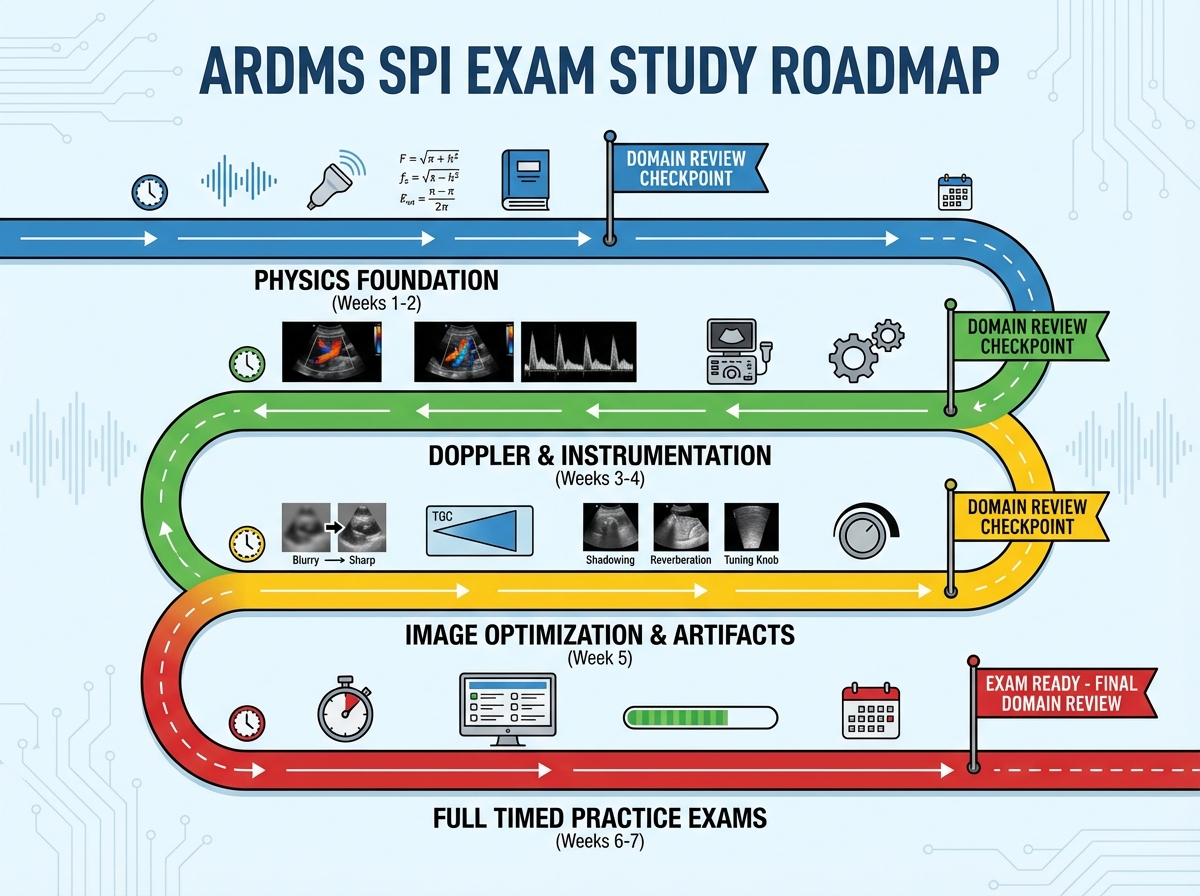
| Physics Foundation | Acoustic principles, pulse-echo, tissue interaction | 1–2 weeks |
| Doppler Mastery | Doppler physics, color/spectral/PW/CW, aliasing, hemodynamics | 1.5–2 weeks |
| Instrumentation & Transducers | Equipment types, controls, knobology | 1 week |
| Image Optimization & Artifacts | Artifact identification and cause-effect reasoning | 1 week |
| Safety, QA, and Patient Care | ALARA, bioeffects, quality assurance protocols | 3–5 days |
| Full Practice Exam Phase | Timed full-length tests, review, weak domain targeting | 1.5–2 weeks |
| Total | 7–9 weeks |
The order of these stages matters more than the speed — building physics logic before attempting Doppler questions makes the Doppler material stick in half the time. If you find yourself at week 10 still not feeling ready, that’s completely normal; the scaled scoring system rewards depth of understanding over coverage speed.
What Passing Actually Requires
The SPI asks you to demonstrate that you think like a sonographer — not that you’ve memorized a textbook. The questions are written to test whether you can apply physics reasoning to real equipment and real clinical decisions. That’s a different cognitive skill than retention.
The candidates who pass on the first attempt aren’t necessarily the ones who studied the most hours. They’re the ones who spent their hours the right way: understanding Doppler deeply, connecting physics to equipment behavior, and practicing under realistic conditions with honest review of every wrong answer. The 71% first-time pass rate means this is genuinely achievable with the right preparation — and genuinely risky with the wrong approach.
Study Doppler first, not last. At 34% of the exam, it’s your biggest score lever — and it takes the longest to internalize because it requires layering multiple physics concepts together.
Draw the Doppler angle diagram by hand. Write out what happens to the cosine value as angle increases toward 90 degrees, and what that does to your velocity calculation. Physical tracing makes this permanent.
Learn every artifact by its physical cause, not its appearance. The exam asks you to reason, not recognize. Know why reverberation produces equally spaced lines and how to eliminate it.
Practice with scaled difficulty. Start with foundational questions and systematically work toward harder scenario-based questions. Skipping to difficult questions early creates false confidence or false discouragement — neither helps.
Aim for 80–85 correct answers, not 78. The scaled scoring system means a slightly harder exam version can fail you at 78 correct. Build a real buffer.
Time yourself aggressively in the final two weeks. Use 65 seconds as your average target but flag calculation questions and return to them — don’t spend three minutes on one question while ten easier ones wait.
Review every wrong answer by rewriting the reasoning. Don’t just read the explanation — write out in your own words why that answer is correct and why the other three options are wrong. This is the fastest way to close conceptual gaps.
Focus QA questions on the “why” behind each protocol. Know why ALARA exists, why thermal index matters more than mechanical index in the third trimester, and why phantom testing validates equipment accuracy — not just the names of the protocols.
Leave a Reply