The first time someone told me my back pain was a breathing problem, I almost walked out of the room.
If you’re looking to learn core stability through breathing, the answer isn’t more crunches or a stronger plank — it’s retraining the deep pressure system inside your trunk that most people never even knew existed. The diaphragm, pelvic floor, deep abdominals, and spinal muscles operate as a single hydraulic unit. When that system breaks down, the body compensates with surface muscles that were never designed to carry the load — and that’s where back pain, neck tension, and restricted movement come from.
- If your back pain returns despite regular exercise, your breathing mechanics — not your muscle strength — are likely the root cause.
- Chronic neck and upper back tightness is often the body’s compensation for a diaphragm that isn’t doing its postural job.
- Retraining core stability through breath takes 4–8 weeks of consistent, low-load practice before the nervous system begins to automate the pattern.
What “Core” Actually Means for Someone With Back Pain
Most people with back or neck pain have been told to strengthen their core — and most of them have tried. They’ve done planks, dead bugs, bird dogs. Some feel better for a while. Many don’t. The reason is almost never effort. It’s a misunderstanding of what the core actually is.
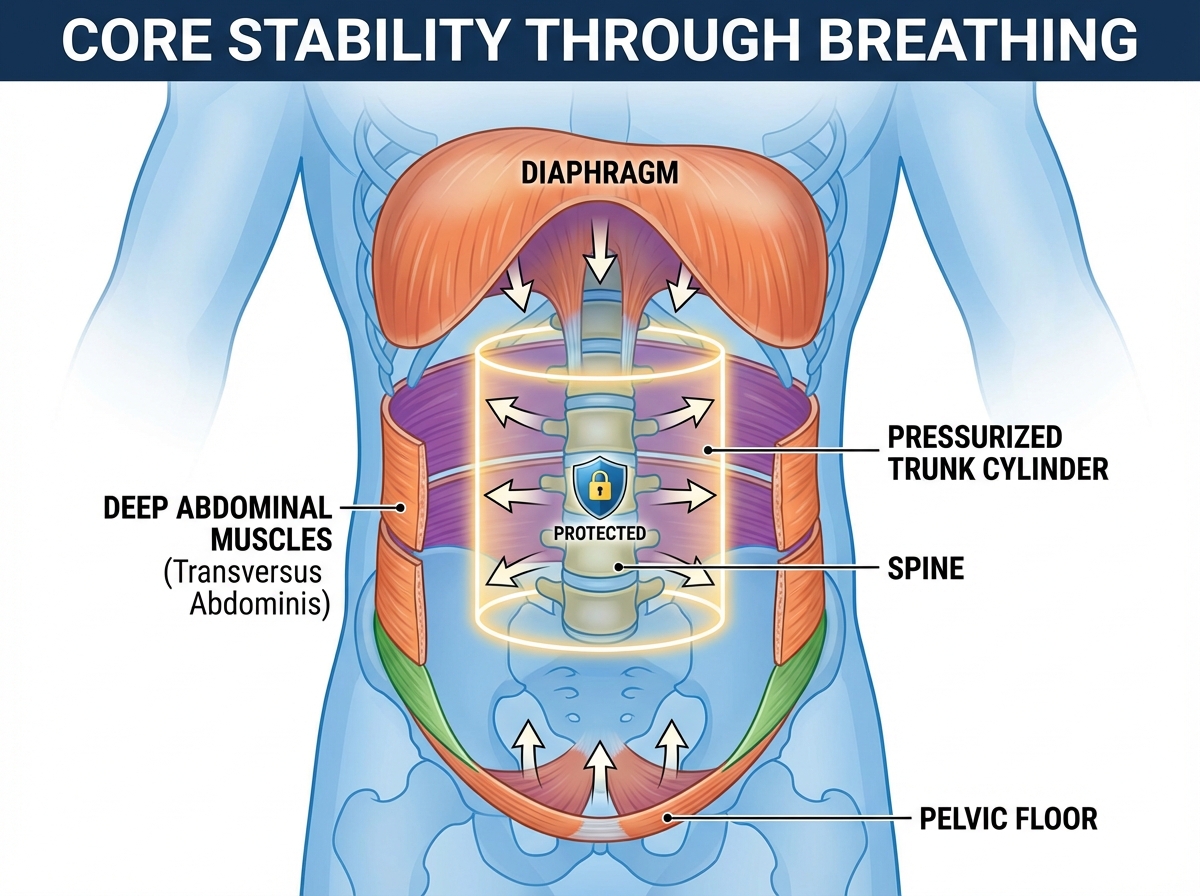
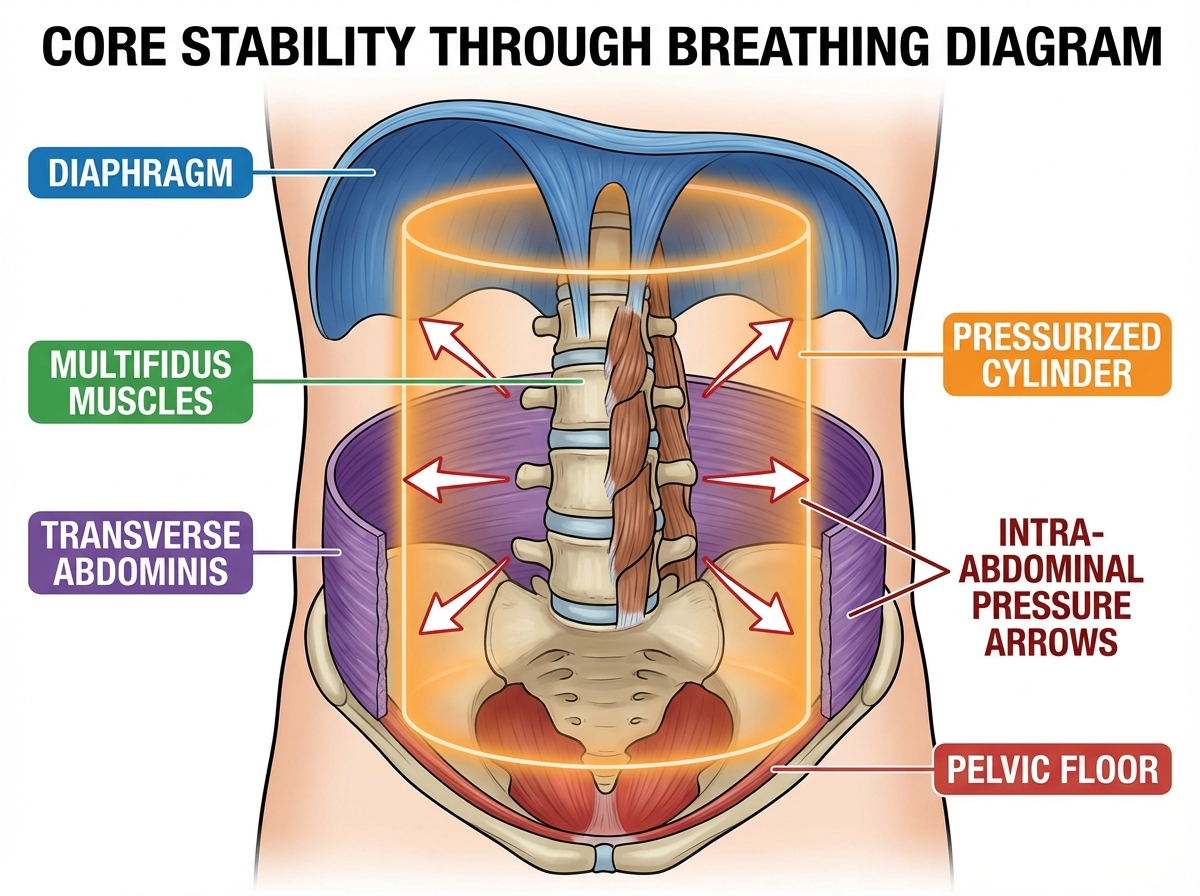
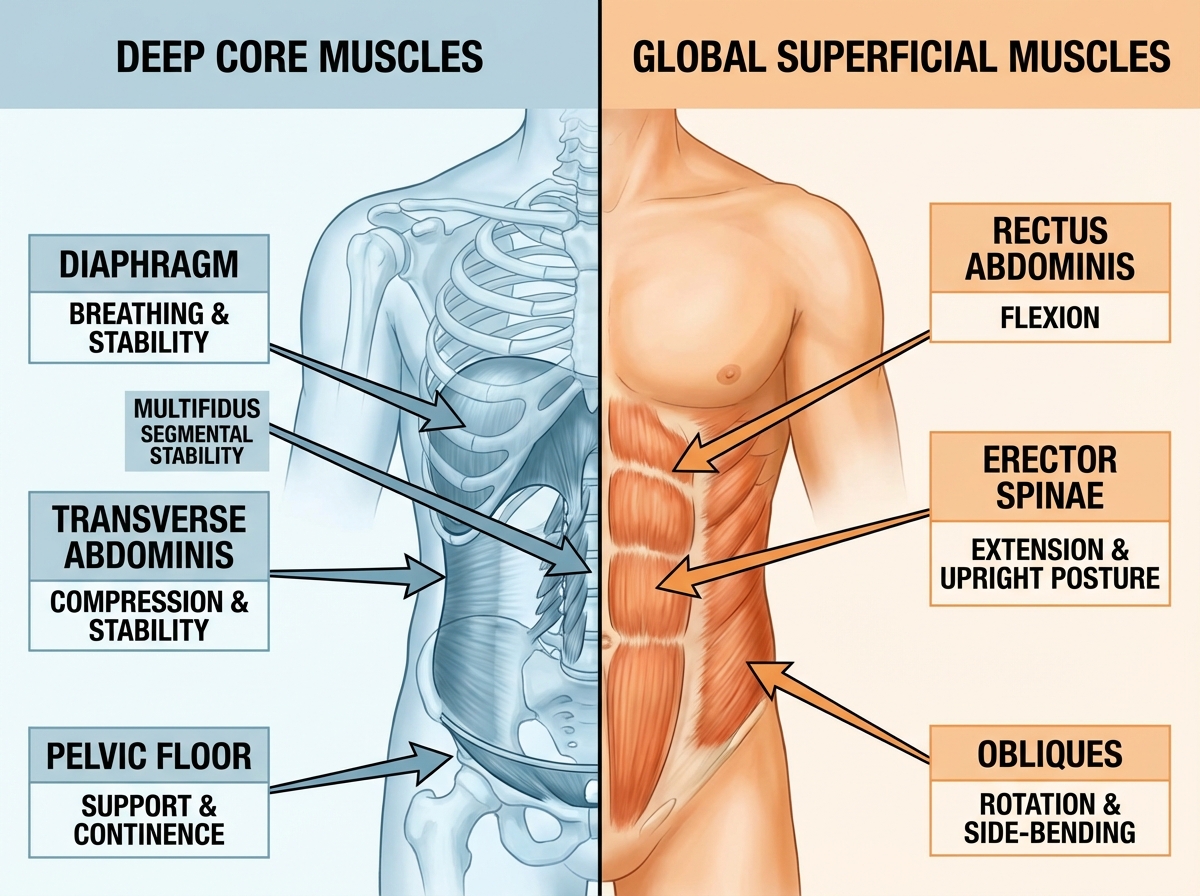
The core is not a set of visible muscles you can flex in the mirror. It’s a pressure chamber. Picture a soda can: strong not because its walls are thick, but because the pressure inside is balanced. Your trunk works the same way. The roof of that chamber is the diaphragm. The floor is the pelvic floor. The walls are the deep abdominals — specifically the transverse abdominis — and the deep spinal muscles called the multifidus. These four structures don’t produce movement. They regulate intra-abdominal pressure, and that pressure is what actually stabilizes your spine.
On top of this deep system sits a second layer — the global muscles. Rectus abdominis, obliques, erector spinae. These are the muscles you feel burning during a crunch. They’re important, but they’re meant for producing force and movement, not holding your spine steady through the day. When the deep system fails, the global muscles take over postural work they weren’t built for. That’s when you get the chronic tightness in your lower back and the tension headaches that creep up your neck by 3pm.
Why Your Rib Cage Is the Part Nobody Talks About
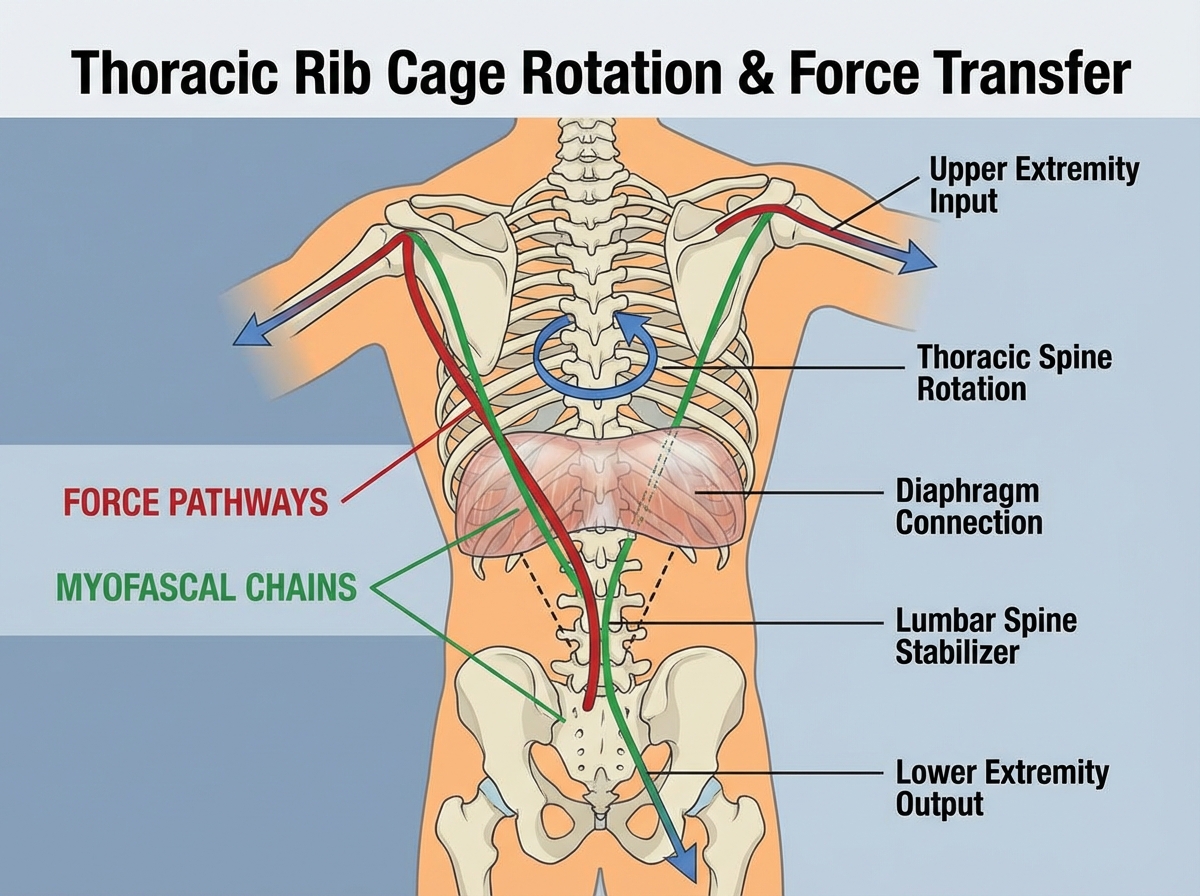
Thoracic anatomy never comes up in most fitness conversations, and that gap is where a lot of chronic pain lives. The rib cage is not just a protective shell for your organs. It’s the structural hub of trunk rotation. Every time you twist to look over your shoulder, reach across your body, or wind up for a throw, the rib cage is the axis through which that force transfers between your upper and lower body.
When the rib cage becomes stiff — which happens almost invisibly over years of sitting, shallow breathing, and poor posture — rotation gets blocked. The body doesn’t stop moving. It routes movement around the restriction, usually through the lumbar spine or the cervical spine. Both of those areas are built for stability and limited rotation, not for picking up the slack from a locked thorax. This is how a stiff mid-back becomes a neck problem, a lower back problem, or eventually both.
The fascial system ties all of this together in ways that even anatomy textbooks undersell. Myofascial connections link the diaphragm directly to the lumbar spine and the pelvic floor. A restriction anywhere along that chain changes tension everywhere else. Someone who can’t take a full lateral breath isn’t just breathing inefficiently — they’re constantly tugging on the structures that stabilize their low back.
The Diaphragm’s Two Jobs — and What Happens When It Can Only Do One
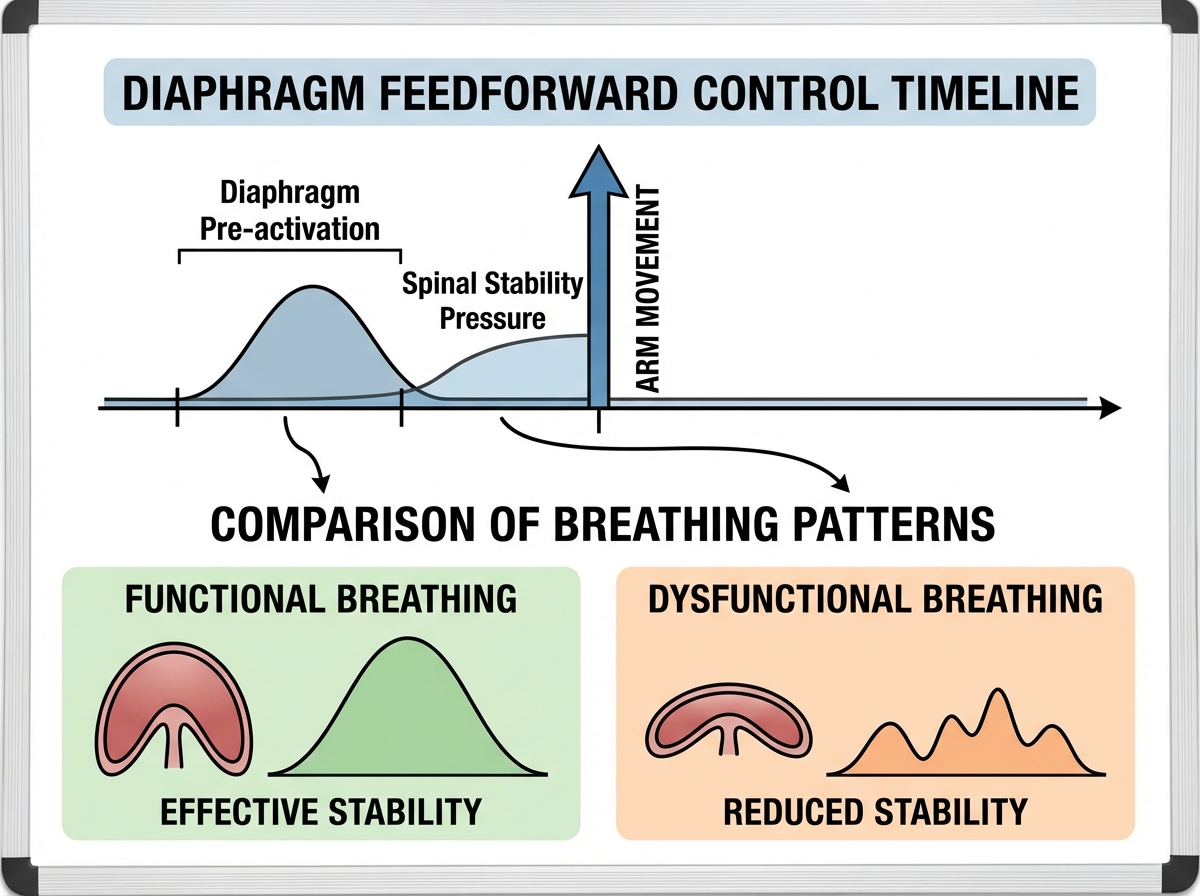
Here’s what most people never learn: the diaphragm has two jobs running simultaneously. It breathes. And it stabilizes your spine. Every time a limb moves — your arm reaches forward, your leg steps off the ground — the diaphragm fires a split second before that movement to pre-pressurize the trunk. This anticipatory response is called feedforward control, and it is the actual mechanism behind spinal protection during movement.
The problem is that when breathing demands increase — stress, poor posture, mouth breathing, a tight rib cage — the body prioritizes ventilation over stability. The diaphragm’s postural role gets demoted. Spinal stability suffers. And because this happens gradually and silently, most people don’t notice the shift until they’re managing chronic pain. For people who have dealt with back issues for years without resolution, this is almost always part of the picture.
Dysfunction in the diaphragm doesn’t announce itself with a dramatic symptom. It shows up as a subtle forward head posture, ribs that flare slightly out, a pelvis that tilts under load, incontinence with jumping or coughing, or a sense of being “not quite stable” on one leg. These are not separate problems. They share a root in compromised diaphragmatic function — and retraining that function is what changes the pattern.
How to Learn Diaphragmatic Breathing for Core Stability
Learning diaphragmatic breathing for core stability starts with one uncomfortable truth: most people are already breathing, and most of them are doing it wrong in a way that feels completely normal. The chest rises. The upper neck muscles work. The belly stays rigid. This is the breathing pattern of a stressed nervous system, and for many people it has been the default for so long that anything else feels strange.
The practice starts supine. Knees bent, back relaxed. One hand on the chest, one just below the navel. Inhale through the nose — not just forward into the belly, but 360 degrees. The lower ribs should expand sideways. The back should press gently into the floor. This is lateral costal expansion, and for most people the sensation of breathing into the sides and back of the rib cage is completely foreign the first time they try it. That unfamiliarity is informative. It’s telling you exactly where the restriction is.
The exhale is where core engagement happens. A slow, controlled breath out through pursed lips engages the deep abdominals, lifts the pelvic floor, and drops the rib cage back down toward neutral. Done properly, this is more core activation than most people get from a set of crunches — with zero compression through the spine.

The Pelvic Floor, Incontinence, and the Connection No One Explains
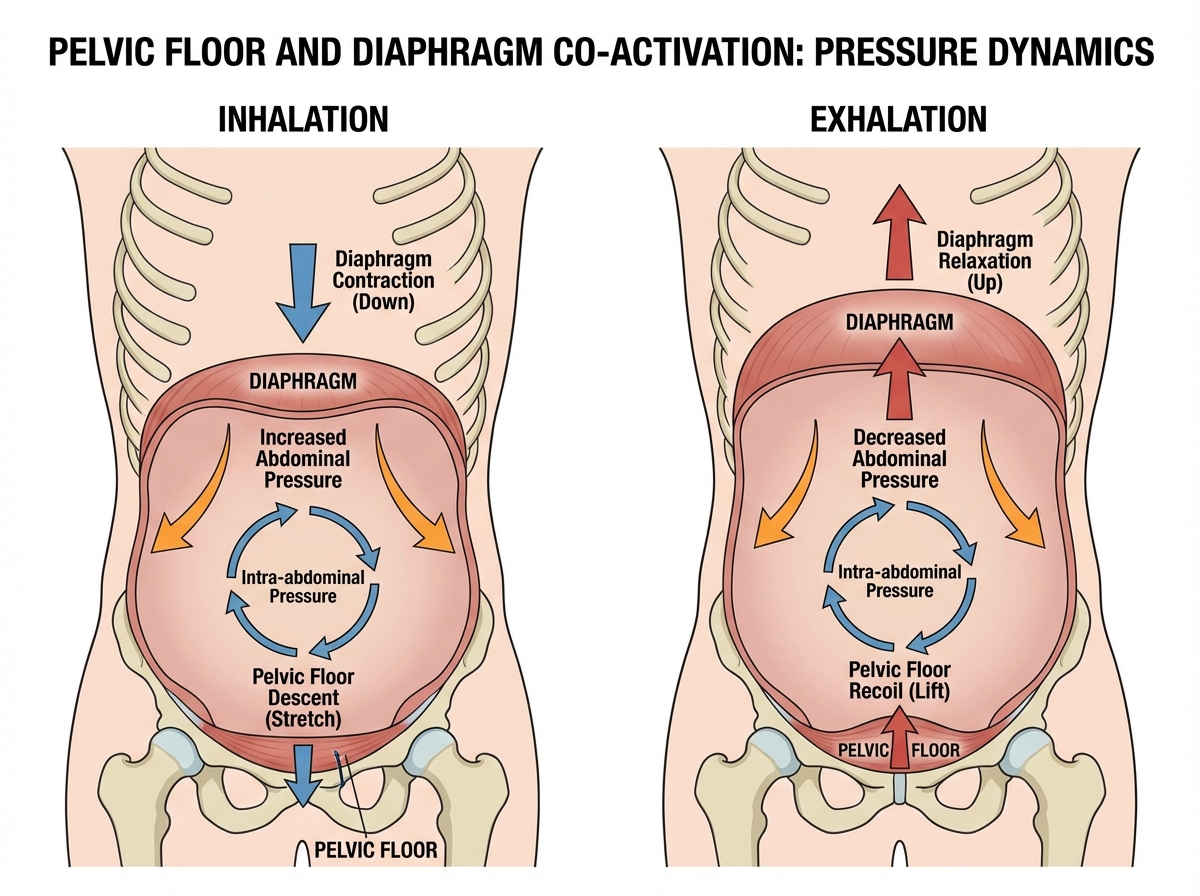
The single biggest mistake people make when trying to improve core stability is treating the pelvic floor and the diaphragm as separate systems. They aren’t. They work in direct mechanical partnership. When the diaphragm descends on inhalation, intra-abdominal pressure rises. The pelvic floor responds by lengthening to accommodate that pressure while maintaining tone. On exhalation, both recoil. If the pelvic floor can’t respond — because it’s too tight, too weak, or not coordinated — the pressure has nowhere to go, and the system loses stability.
This is why incontinence on impact — leaking when you cough, jump, or sneeze — is a core stability problem, not just a pelvic floor weakness. The pelvic floor isn’t failing in isolation. The whole pressure management system is out of sync. And it’s also why aggressive kegel protocols alone rarely fix the problem: you’re strengthening one part of a system without reintegrating it with the rest.
For people with scoliosis, this relationship becomes even more complex. Asymmetrical rib cage mechanics and uneven diaphragm excursion create predictable patterns of compensation through the entire trunk. Addressing the breathing mechanics — not just the spinal curve — is what changes the functional picture.
How Long It Actually Takes to Rewire This
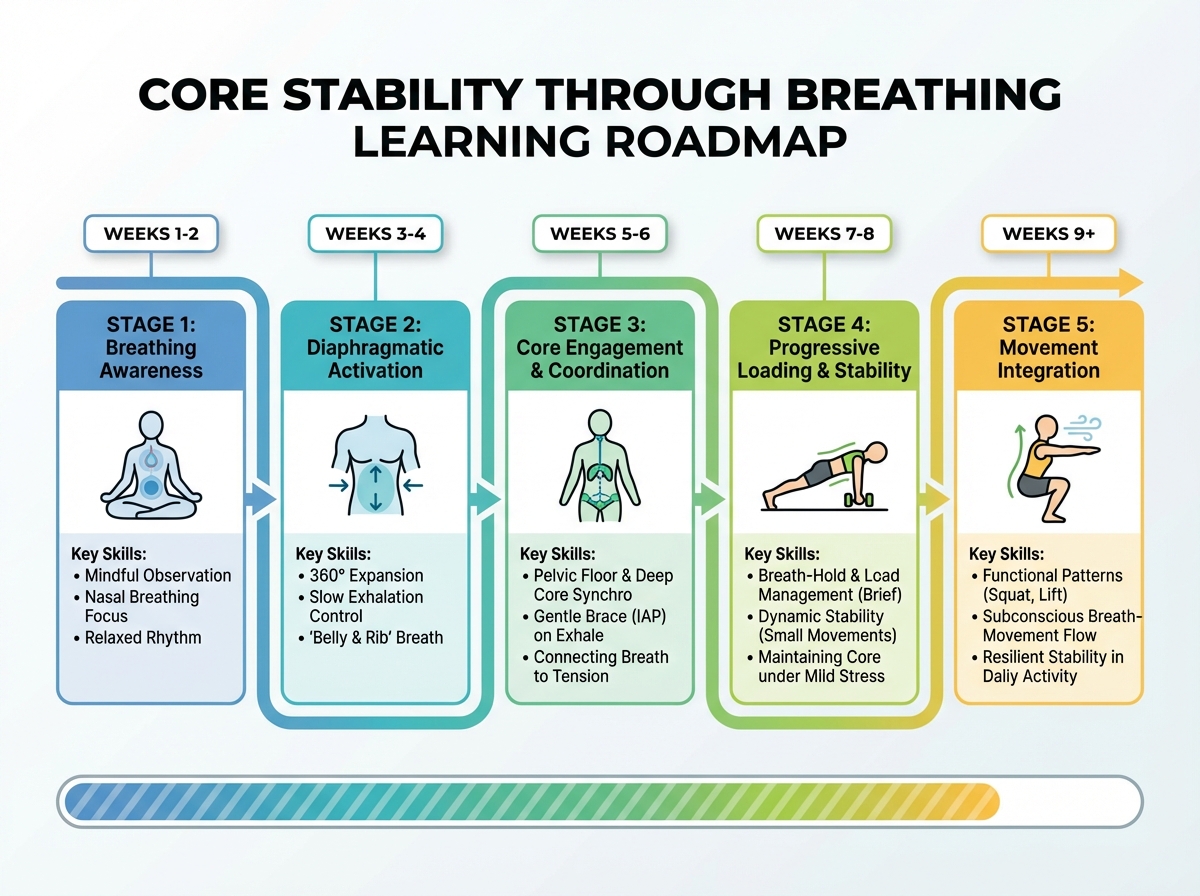
| Stage | Content | Estimated Time |
|---|---|---|
| Awareness | Recognizing existing breathing pattern, learning 360-degree breath | Week 1–2 |
| Lateral Costal Training | Practicing lateral rib expansion, three-sniff technique, balloon breathing | Week 2–3 |
| Deep Core Facilitation | Supine breathing reach, core facilitation drills, pelvic floor coordination | Week 3–5 |
| Loaded Integration | Modified Pilates 100, trunk rotation with breath, strength testing | Week 5–8 |
| Movement Patterns | Lengthening drills, lateral trunk rotation with inspiration, functional carryover | Week 8–12 |
| Total | Full pattern reintegration into daily movement | 10–12 weeks |
Order matters far more than speed here — layering trunk rotation before the basic pressure system is reliable will just reinforce the compensations you’re trying to fix. And if you find yourself taking 14 or 16 weeks to feel confident at each stage, that’s not falling behind — that’s how long a nervous system takes to change a pattern it’s been running on for years.
What Changes When You Start Breathing Correctly
The first change most people notice isn’t less pain. It’s a different quality of stillness. Standing feels more grounded. Sitting upright for longer doesn’t produce the familiar pull across the lower back. The neck stops working as a substitute stabilizer when you reach for something. These are small things, but they matter because they signal that the deep system is coming back online — doing the low-level stabilizing work it was supposed to be doing all along.
The second shift is in how movement feels. Trunk rotation — which had been stiff and guarded — starts to open up. The rib cage begins to move with you instead of against you. Reaching overhead doesn’t compress the neck. Walking has a different quality; the pelvis transfers force more efficiently, and the lower back stops bracing against every step.
For people who have been managing chronic neck pain, the connection to breathing mechanics can feel almost implausible at first. But the cervical spine sits directly above the rib cage. When the thorax is locked, the neck takes over rotation demands it wasn’t designed to handle. Restoring thoracic mobility through better breathing mechanics is one of the most reliable ways to reduce chronic neck tension — often more effective than any amount of direct neck treatment in isolation. For those working through persistent neck discomfort alongside these exercises, exploring lower back pain relief with core stabilizer exercises can provide additional strategies that complement the breathing work.
When Obesity, Breathing, and Core Function Intersect
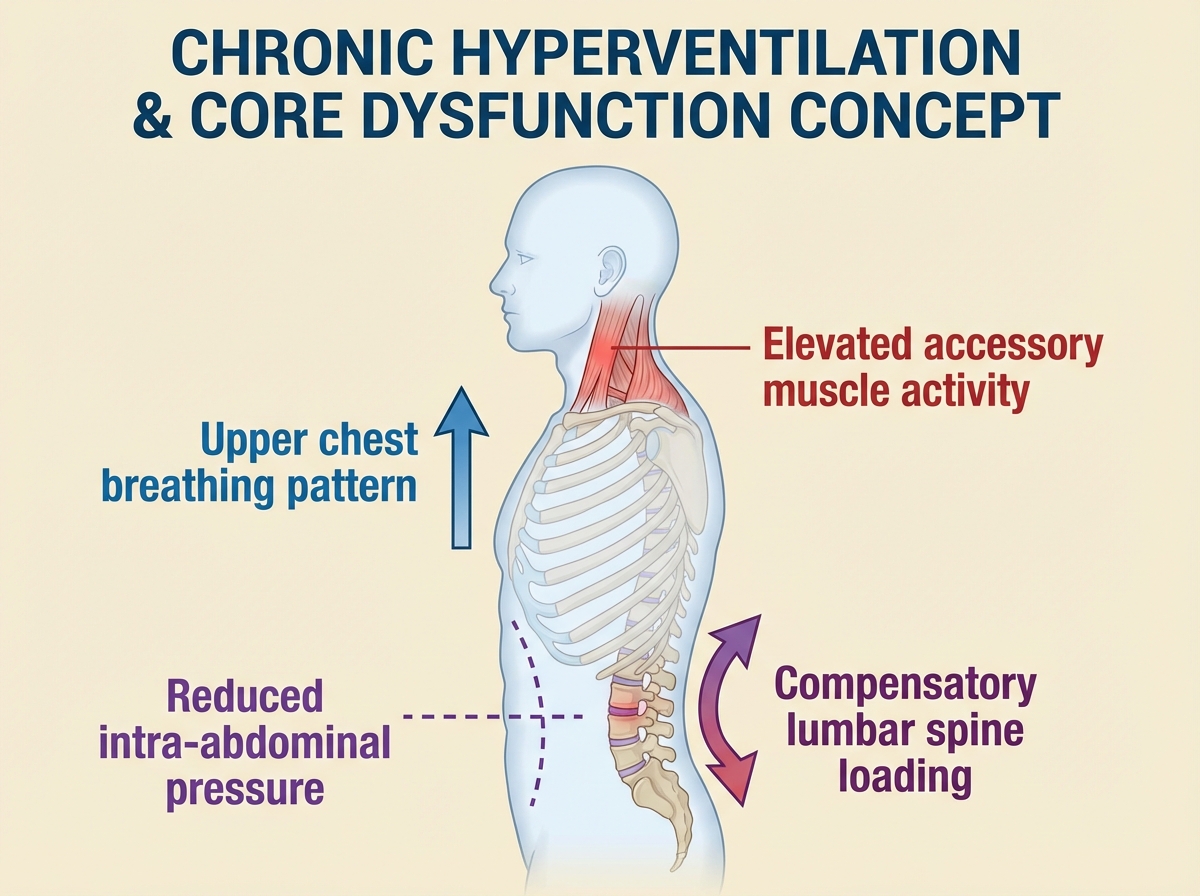
Excess abdominal weight changes the mechanical environment of the diaphragm in ways that compound every problem described above. The diaphragm’s ability to fully descend on inhalation is physically limited. Intra-abdominal pressure is already elevated at rest, which means the system is perpetually pre-loaded without the coordinated muscle engagement to manage it. Breathing becomes predominantly upper chest. The deep core progressively loses its role in stability.
This isn’t a moral observation — it’s a mechanical one, and it applies to anyone whose diaphragm is working in a compromised position. The same basic pattern occurs in advanced pregnancy, after abdominal surgery, and in people who have developed chronic hyperventilation as a stress response. In all of these cases, the pathway back is the same: start with awareness of the breathing pattern, restore the rib cage mechanics, rebuild the deep system from the inside out.
The exercises that support this rebuild are deliberately low-load and position-dependent. Lateral costal expansion facilitation, supine breathing reach, the three-sniff technique — none of these look impressive. None of them belong in a motivational highlight reel. But they are the specific inputs a compromised nervous system needs to reconnect with a deep core that has been outsourced to the wrong muscles for years. For those dealing with persistent low back issues alongside these breathing patterns, understanding how to treat your own back pain and sciatica at home can provide a useful parallel track.
The Triple Core Concept and Why It Changes Everything
The “triple core” framework reframes the entire conversation about trunk stability. Instead of thinking about the core as a set of muscles to strengthen, it positions the trunk as three stacked regions — thoracic, lumbar-abdominal, and pelvic — each needing to move and stabilize in coordination with the others. When one region is locked or overloaded, the other two compensate. Restoring function means restoring communication between all three.
This framework is practical because it explains clinical observations that don’t make sense in a simpler model. Why does stretching the hip flexors help someone’s back? Because pelvic position influences lumbar loading. Why does rib cage mobility matter for shoulder pain? Because thoracic restriction forces the scapula to compensate. Why does breathing retraining reduce neck tension? Because the cervicothoracic junction can’t do its job when the thorax isn’t moving properly below it.
Understanding the triple core concept doesn’t require memorizing anatomy. It requires recognizing patterns: where is the system bracing? Where has movement stopped? Where is the compensation showing up? Once you start seeing movement through that lens, the logic of breathing-based core stability training becomes obvious. If you’re also working on general rehabilitation with a structured, layered approach, exploring how to relieve lower back pain with core stabilizer exercises applies this same stacked-systems thinking to targeted movement rehab.
What to Do With This Right Now
Practice lateral costal breathing before any other core exercise — place your hands on your lower ribs and try to push them sideways on inhalation. If you can’t, that’s your starting point, not planks.
Use the three-sniff technique to wake up the diaphragm — three short inhalations through the nose followed by a long exhale activates the diaphragm more reliably than a single deep breath for most people relearning the pattern.
Try blowing up a balloon once per day — the resistance of expiration against pressure forces the deep abdominals and pelvic floor to coordinate in a way that no verbal cue can fully replicate.
Do your breathing practice in different positions — lying down, seated, standing, and finally during slow walking. The nervous system needs to relearn the pattern in each position separately.
Stop sucking in your stomach as a stability strategy — drawing the navel to the spine reduces intra-abdominal pressure, the opposite of what creates spinal stability. Bracing (gentle outward pressure in all directions) is the correct cue.
Test lateral trunk rotation with an inhale — on your next rotation stretch, try inhaling as you rotate rather than exhaling. The expansion of the rib cage during inhalation mechanically assists thoracic rotation in ways that exhale-based stretching doesn’t.
Notice where your neck tightens during effort — neck bracing during exertion is a direct sign that the deep core is not pre-activating and the body is routing stabilization through the wrong structures.
Give the pattern six weeks before judging it — the nervous system changes slowly. The absence of dramatic early results is not a signal that the approach is wrong. It’s the timeline of genuine neuromotor retraining.
Leave a Reply